
Percutaneous Vegetation Removal Immediately Preceding Lead Extraction: A New Approach to Treating CIED Related Endocarditis
2Interventional Radiology, Montefiore Medical Center
Aim: Cardiac implantable electronic device (CIED) lead extractions are becoming increasingly prevalent. Management of CIED infections in patients with large vegetations poses unique safety and efficacy challenges. There are limited reports of removing vegetations in separate procedures prior to CIED extraction. We present a case of a patient with endocarditis with multiple large vegetations who underwent debulking of the vegetations followed immediately by percutaneous lead extraction.
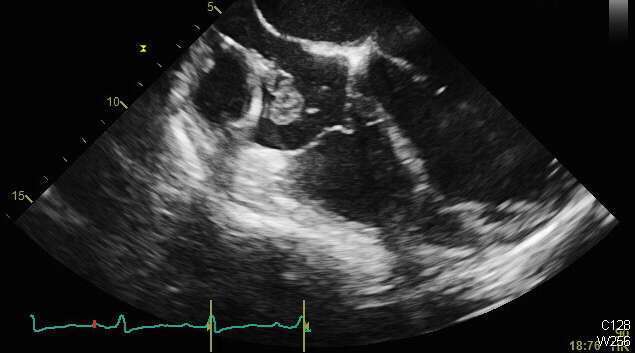
Methods and Results: A 56-year-old male with a dilated CM, underwent dual chamber ICD implantation 15 years earlier and placement of a pace-sense lead 3 years prior to presenting with Staphylococcus epidermidis bacteremia. A TEE demonstrated multiple large vegetations adherent to the leads, with the largest vegetation measuring 3x2cm. Given the risk of embolization, a decision was to attempt endovascular removal of these vegetations prior to lead extraction.
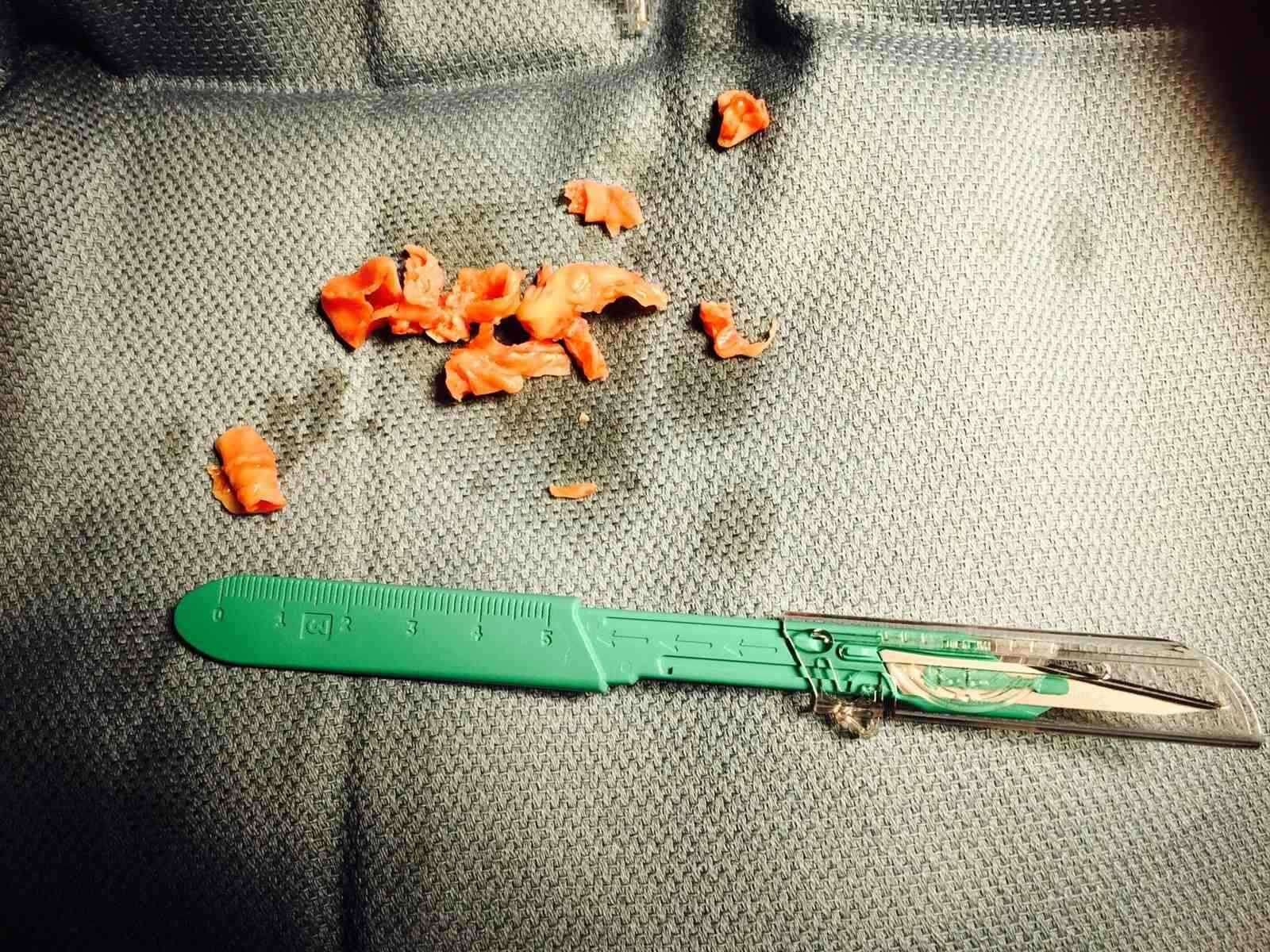
The Angiovac system comprises a circulatory pump circuit that is connected to a 22F venous drainage cannula that was inserted via the right IJ and a reinfusion cannula placed via the right femoral vein. TEE guidance was used to position the Angiovac cannula proximate to the vegetations and multiple large fragments were removed, while small residual vegetations adjacent to tricuspid leaflets remained in situ even after lead extraction.
As full heparinization is required during the Angiovac procedure, anticoagulation was then reversed. Immediately following reversal, successful extraction of all three leads was performed in the same setting so as to avoid the need for serial procedures on different days. Patient had no clinically recognizable pulmonary embolization and remained hemodynamically stable throughout.

Conclusion: A combined approach of endovascular removal of large masses immediately preceding lead extraction is feasible, may offer safety advantages and enhance clinical outcomes of patients with CIED related endocarditis.
Powered by Eventact EMS