
Severe Familial Hypercholesterolemia: Prevalence and Characterization of Patients Presenting for Cardiac Catheterization
2Director, Clalit Health Services, Haifa and Western Galilee District
3Department of Medicine, Lady Davis Carmel Medical Center, Haifa
4Ruth and Bruce Rappaport Faculty of Medicine, Technion - Israel Institute of Technology, Haifa, Israel
Background: Patients with severe familial hypercholesterolemia (FH) are often unrecognized despite typical presentation. Patient identification is important, as early intensive treatment and cascade screening of families may reduce event rates. Screening of medical databases may enhance identification, characterization and management of severe FH patients.
Methods: Retrospective analysis of cardiac catheterization laboratory database between the years 2002-mid 2015 was performed. Patients presenting for catheterization with LDL-C level ≥130mg/dl (n=2,383) were screened for presence of severe FH, defined as any past documentation of LDL-C ≥280mg/dl. Patient characteristics, peak and current LDL-C levels and lipid-lowering therapies were evaluated. Initial cascade screening of families was performed using HMO database.
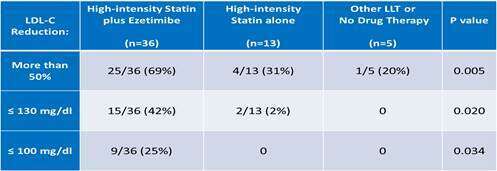
Results: Severe FH was noted in 54 patients (prevalence 1:44 of patients screened; 20% females). Mean age at initial diagnosis of cardiovascular disease (CVD) was 45 years (range 27-67). Peak LDL-C was 280-464 mg/dl (median 322, IQR 295-349). Coronary bypass surgery (CABG) was performed in 26 (48%), and redo CABG in 5 (9%). Additional risk factors included obesity (33%), hypertension (59%), current smoking (33%) and diabetes mellitus (24%). LDL-C reduction ≥50% was achieved in 30 (56%); LDL-C<130mg/dl in 17(32%), and LDL-C<100mg/dl in 9 (17%) . High-intensity statin plus ezetimibe was prescribed in 36 (67%), statin alone in 13 (24%) and other lipid-lowering therapies or lack of treatment in 5 (9%). Concomitant plasmapheresis was performed in 2 patients. The intensity of treatment was directly associated with attainment of LDL-C goals (Table). Preliminary review of laboratory data of family members has identified >150 additional individuals with possible FH.
Conclusions: Retrospective analysis of a large catheterization database revealed patients with severe FH and coronary disease at a young age, with low attainment of cholesterol treatment goals. Systematic screening of large databases of populations at-risk will promote identification and management of severe FH patients and their affected family members.
Powered by Eventact EMS