
The Escalation and Mortality Dilemma in The Eyes of CTPA
2Radiology Department, Sheba Medical Center
3Non Invasive Cardiology Unit, Sheba Medical Center
4Invasive Cardiology Unit, Sheba Medical Center
Background: The increasing occurrence of pulmonary emboli (PE) sets a substantial dilemma for the treating physician. The most challenging group of patients is the intermediate risk PE patients according to the European society of cardiology (ESC), in whom clinical deterioration might cause demise. Our goal was to evaluate whether parameters derived from chest CTPA angiography at presentation can predict clinical outcomes.
Methods: The study comprised 170 consecutive patients admitted to the ICCU due to ESC intermediate or high risk PE. PE was diagnosed based on CTPA findings. The following volumetric measurements were determined in admission chest CTPA: Right and left ventricular volumes and their ratio (RV/LV), right and left atrial volumes and their ratio (RA/LA), main pulmonary artery diameter (MPA) and the presence of contrast reflux to the IVC. The primary end-point was a combined end point of mortality and\or subsequent need for escalation therapy (thrombolysis, mechanical ventilation or catecholamine support).
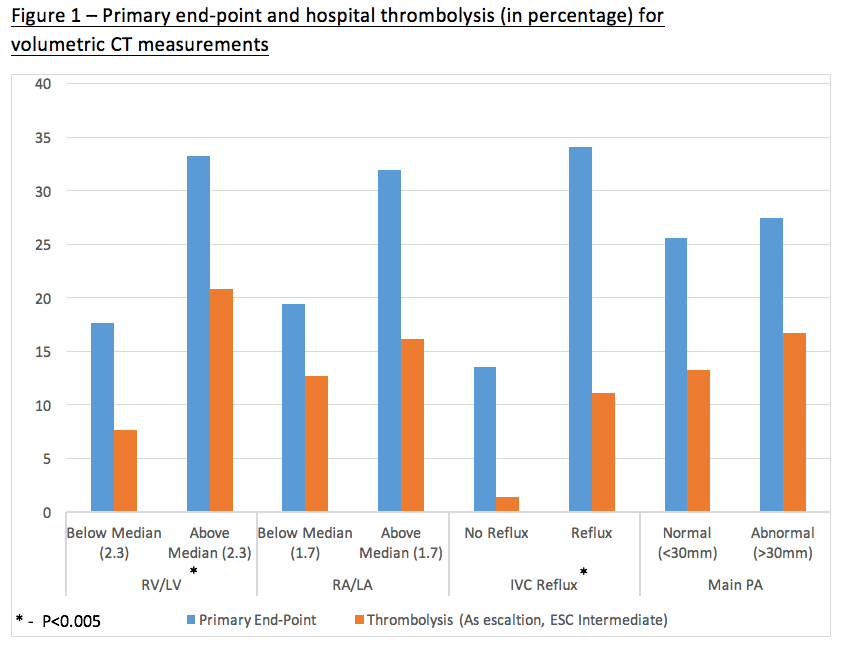
Results: Among the entire study population 46 (27%) patients sustained the primary end-point, 22 (12.9%) received thrombolysis and 14 (8.2%) have died during their in-hospital course. When stratified into two groups using median RV/LV ratio (2.3), those with higher RV\LV ratio were more likely to sustain the primary end-point (33% vs. 18%, p=0.04). Furthermore, ESC intermediate risk patients with above median RV\LV had higher change to receive thrombolysis during hospitalization (12% vs. 2.3%, p=0.014). Similarly, IVC reflux on admission CTPA predicted a worse prognosis with higher occurrence of the primary end point (34% vs. 14%, p<0.01) and thrombolysis (11% vs. 1.4%, p=0.02). On the contrary, RA/LA ratio and MPA diameter did not carry any prognostic value. (Figure 1).
Conclusions: Our findings suggest that CTPA based RV/LV ratio and IVC reflux may serve in prognostication and therapeutic guidance, especially for thrombolysis administration, in patients with intermediate risk PE.
Powered by Eventact EMS