
Abnormal Multilayer Myocardial Mechanics in Genotype-Positive Left Ventricular Hypertrophy-Negative Patients with Hypertrophic Cardiomyopathy
2Department of Cardiology, Papworth Hospital NHS Foundation Trust, Cambridge
3Cardiovascular Division, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts
4Cardiology, Rambam Health Care Campusl; Technion - Israel Institute of Technology, Haifa
Background: It is unknown whether the presence of a sarcomeric mutation alone is sufficient to results in abnormalities of myocardial force generation, or whether the characteristic changes in myocardial architecture such as hypertrophy, disarray, and fibrosis are required in addition to impair systolic function. Speckle tracking echocardiography allows the quantification of global strain and strain rates, twist and dyssynchrony. We sought to elucidate early abnormalities of myocardial mechanics in carriers of sarcomeric mutations without evidence of clinical disease.
Methods: Sixty genotype-positive left ventricular hypertrophy-negative (G+LVH-) patients with pathogenic mutations in one of the sarcomere genes were compared to 60 normal controls. Velocity Vector Imaging was applied retrospectively to echocardiographic images to quantify global longitudinal and circumferential strain, strain rate, and rotation.
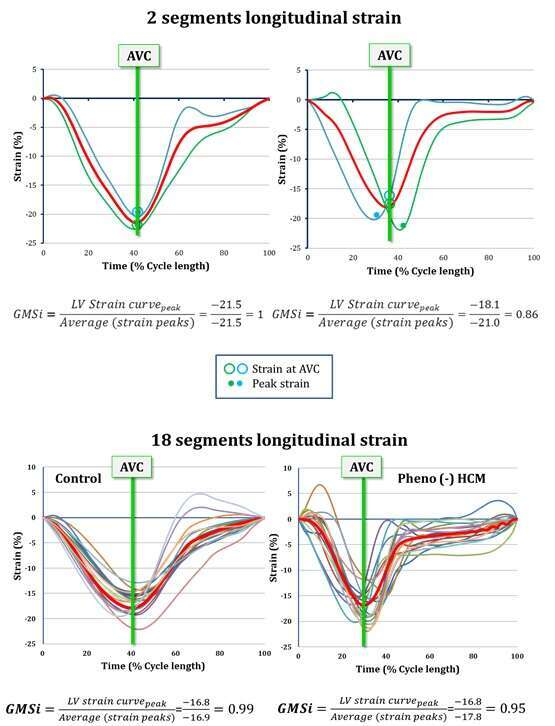
Results: The G+LVH- group demonstrated smaller LV diastolic cavity dimensions (4.5±0.6cm vs 4.8±0.4cm) and higher LVEF (66±6% vs 60±5%) compared with controls. There was an increase in circumferential subendocardial systolic strain in the G+LVH- group (-30±5 vs -27±3%). Both systolic and diastolic subendocardial strain rate were increased in the G+LVH- group compared with controls. Peak rotation angles were higher than normal at the base and apex, with an increase in total twist in the G+LVH- group (11.8±5.6 vs 9.5±4). In the normal group, global strain and average segmental strain were similar, suggesting no or minimal dyssynchrony (GMSi of 0.97-0.98 for all myocardial layers). In the G+LVH- group GMSi was significantly lower, with a subendocardial GMSi of 0.95 and a subepicardial GMSi of 0.60, suggesting the presence of increasing subendocardial to subepicardial dyssynchrony.
Conclusions: In the present study, assessing multilayer strain, we demonstrate that G+LVH- subjects have enhanced subendocardial systolic strain rate and twist, as well as mechanical dyssynchrony within the left ventricular myocardium. These results demonstrate that abnormalities in myocardial mechanics precede the development of clinical hypertrophy.
Powered by Eventact EMS