
Flow Acceleration Time for the Diagnosis of Severe Aortic Stenosis
Background: Current echocardiographic diagnosis of the severe aortic stenosis (AS) is based on valve gradients (peak velocity ≥ 4m/sec or mean gradient ≥40mmHg) and area calculation (≤1 cm2 or index valve area ≤0.6 cm2/m2). Stenotic aortic valve has a characteristic systolic flow pattern with late peaking velocity which can be a helpful parameter in assessing severity of challenging cases. Our aim was to describe systolic time parameters and their diagnostic potential in severe AS.
Methods: A total 150 patients (Mean age 80.13 years, 53% men) with different degrees of AS were studied - 50 for each AS group: mild, moderate and severe. All had normal ejection fraction (≥50%) with no significant other valvular conditions. Systolic time intervals were studied; acceleration time (AT) defined as the time from the beginning of systolic flow to maximal velocity, ejection time (ET) defined as the time from onset to end of systolic flow. The relation of AT/ET was calculated as well.
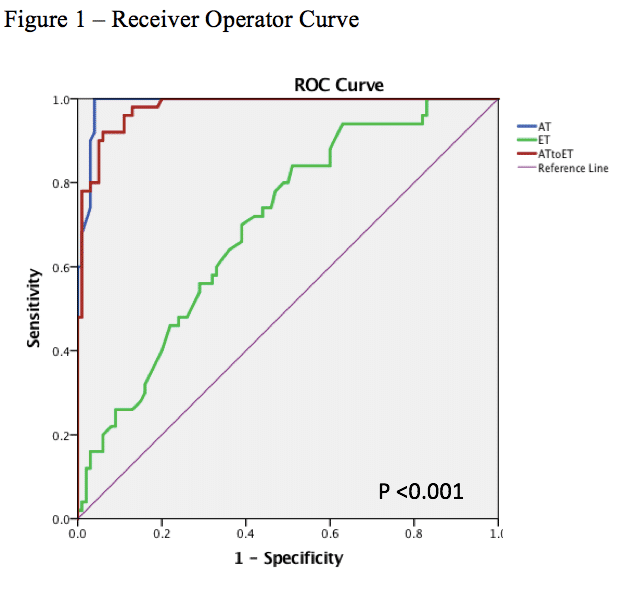
Results: AT was significantly longer for patients with severe AS (80.88±11.91 msec, 86.86±12.09 msec and 133.00±21.32 msec for mild, moderate and severe AS respectively, p<0.001). ET was increased for severe AS (306.82±35.57 msec, 293.67±41.32 msec and 327.28±30.38 msec for mild, moderate and severe AS respectively, p=0.005). AT/ET ratio was larger for severe AS (0.26±0.04, 0.30±0.04, and 0.41±0.05 for mild, moderate and severe AS respectively, p<0.001). Receiver-operator characteristic curve (ROC) analysis has shown that AT and AT/ET can identify patients with severe AS (figure 1). AT > 107.5 msec has shown sensitivity 100% and specificity 96% (area ROC 0.99). While AT/ET ratio > 0.35 had sensitivity 92% and specificity 93% (area ROC 0.98).
Conclusion: AT and the ratio of AT/ET are reliable measurements for identifying patients with severe AS. Those measurements are not angle dependent and can have additive value in challenging cases.
Powered by Eventact EMS