
Chest Pain in the Emergency Room: An Interesting Case Presentation
The use of CCTA for triage of individuals who present to the emergency room with chest pain is an attractive option for community Hospitals. The very high negative predictive value of this modality in low to intermediate risk patients allows for a high percentage of this group to be discharged safely from the emergency room. Patients with moderate CAD can be screened by exercise or myocardial perfusion testing, and critical disease can be directed to the cardiac catheterization lab for intervention.
CCTA screening, properly performed, may result in a decrease in unnecessary admissions and more precise treatment for those patients who are identified with coronary artery disease.
Most patients with coronary atherosclerosis detected by CCTA have readily discernible disease making the distinction between normal and abnormal fairly routine. In the first 6 months of an emergency room CCTA triage program for chest pain in our community hospital we had an interesting patient encounter that illustrates that this is not always the case.
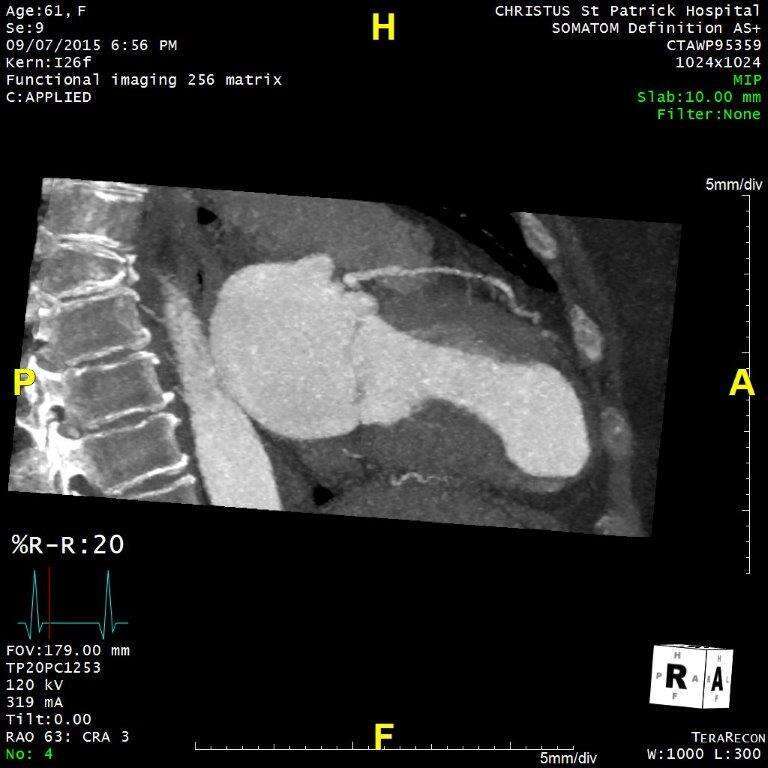
A 61-year-old female presented to the emergency room with atypical chest pain, non-diagnostic electrocardiogram, and a normal initial troponin level. She was referred for CCTA, and on initial review the study appeared to be normal. (Figure 2) However, review of the functional data documented a clearly visible apical wall motion abnormality. (Figures 3 and 4) On closer examination there was a flush occlusion of the distal LAD, with no other coronary artery disease present. (Figure 3)
In this case, the wall motion information drew our attention to the subtle distal LAD occlusion. Assuming functional data can be obtained at reasonably low radiation doses, it may well prove complimentary to images of the anatomy in some cases.
CCTA triage of emergency room chest pain can result in decreased cost and hospital utilization without compromising patient safety. This case illustrates it can be easy to miss significant disease in this setting, particularly if left ventricular function and wall motion informationare not avaliable.
Figure 1: 3D volume rendered image
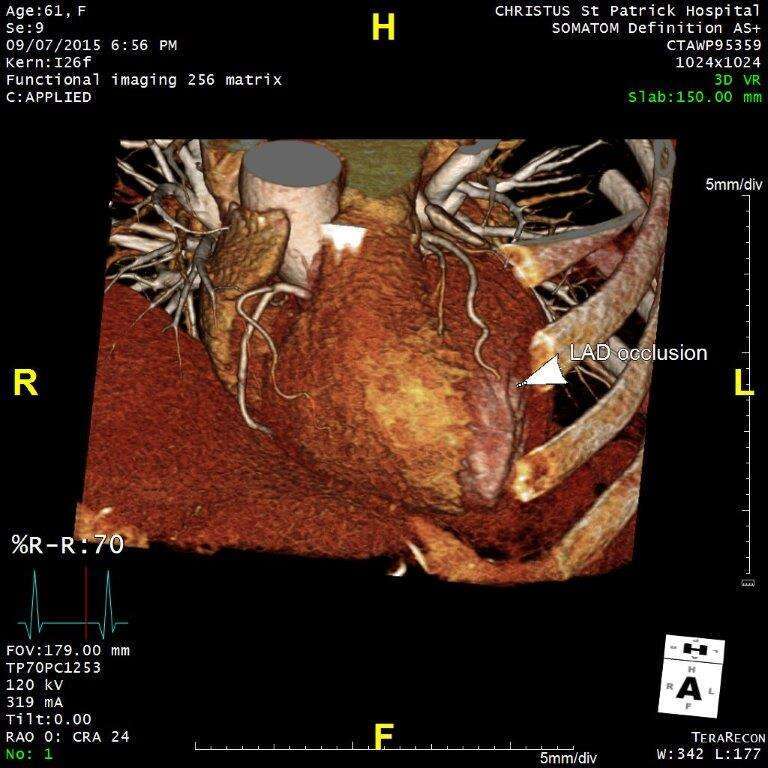
Figure 2: Maximal intensity projection- LAD
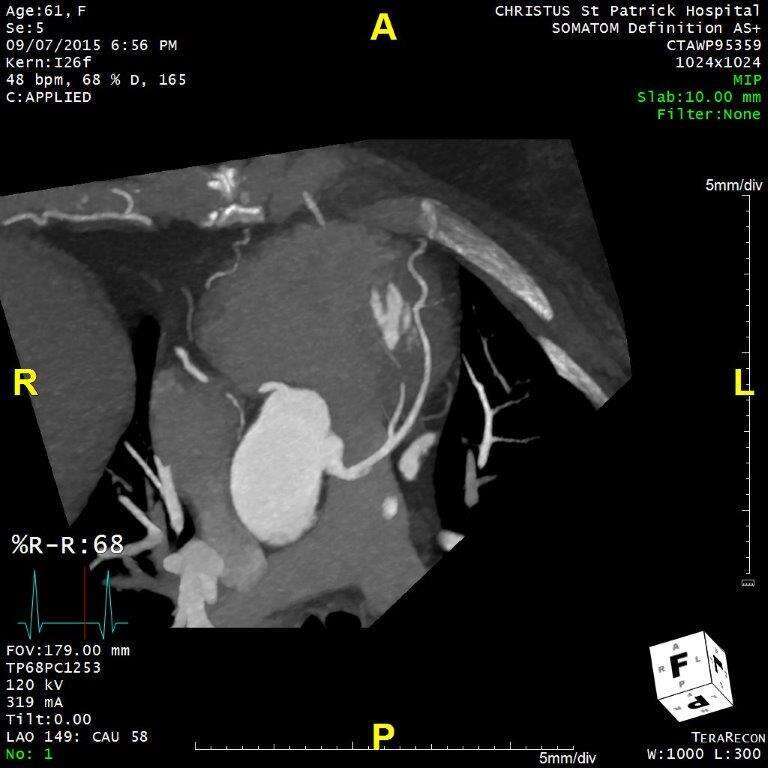
Figure 3: Maximal intensity projection- diastolic frame
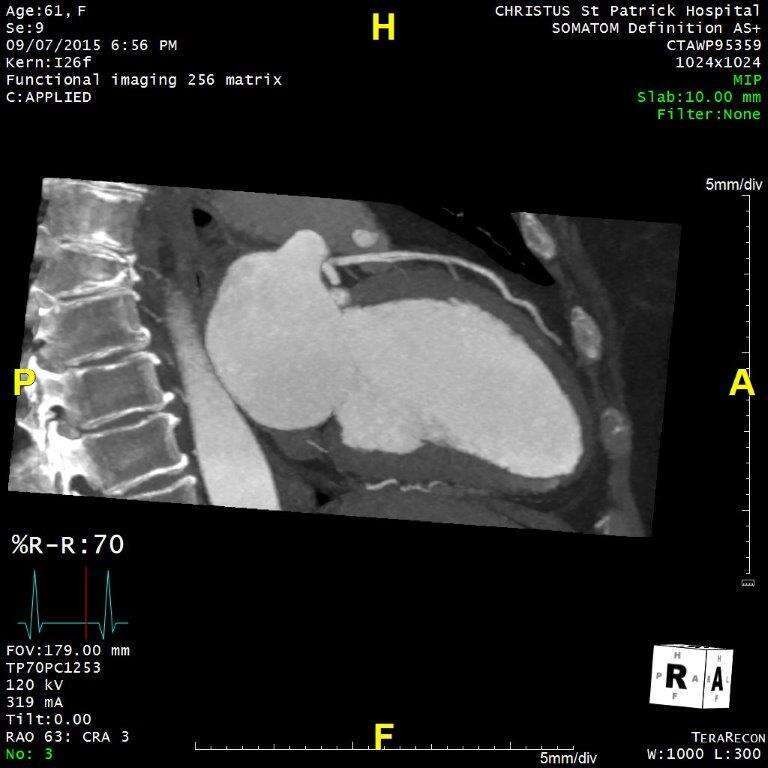
Figure 4: Maximal intensity projectio- systolic frame
Powered by Eventact EMS