
Trends in Frequency and Prognosis of Post Myocardial Infarction Pericarditis in Israel: ACSIS 2000-2013
2Sackler Faculty of Medicine, Tel-Aviv University
3The Leviev Heart Center, Sheba Medical Center
Introduction:
Early post myocardial infarction pericarditis (PMIP), pericardial effusion and Dressler syndrome are the major pericardial complications after acute myocardial infarction (AMI). There are scarce data regarding the incidence and prognosis of early PMIP in the modern era.
Objective:
To assess the incidence and prognostic impact of early PMIP in the contemporary era of aggressive coronary reperfusion.
Methods:
A retrospective analysis of all patients with acute coronary syndrome (ACS), included in the ACSIS 2000-2013 registry database was performed. The primary outcome was major adverse cardiovascular events (MACE), defined as the composite of all-cause mortality, non-fatal myocardial infarction, cerebrovascular event, stent thrombosis or revascularization. The secondary outcomes were mortality and length of stay (LOS) during the acute hospitalization.
Results:
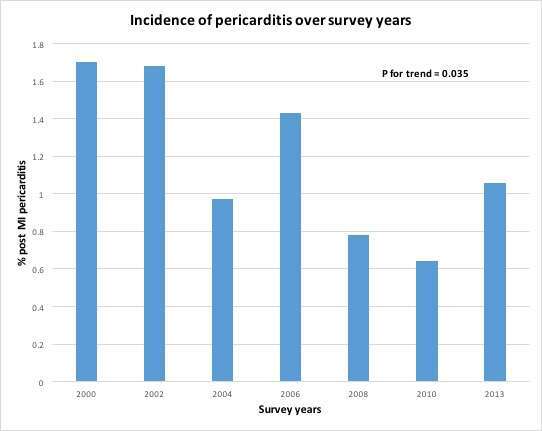
Overall 90 patients (0.67%) of 13,387 patients had PMIP. Most of the PMIP occurred after STE-ACS (84.4%). Further only STE-ACS group was analyzed. PMIP incidence gradually decreased from 170 per 10,000 in 2000 to 110 per 10,000 in 2013, respectively (35% reduction, P for trend=0.035 [figure]).
STE-ACS patients with PMIP were younger (median [IQR]) 58.0 [51.0-65] vs. 61.0 [52.0-72.0]; P=0.045), and had less hypertension. Cardiac biomarkers (troponin T/I and CK) were significantly higher and reduced LVEF was more frequent (87% vs. 67%; P=0.001) in PMIP versus no PMIP group, respectively). PMIP patients had longer time to reperfusion (225min [155-420] vs. 183min [125-300]; P=0.016) and longer LOS (7.0 vs. 5.0 days; P<0.001). PMIP independently predicted MACE for 30 days in a univariate (OR=3.34, 95% CI 2-5.45) and after propensity score matching analysis (OR=2.98, 95% CI 1.53-5.75). There was no significant difference in 1 and 5-year survival.
Conclusion:
PMPI is a relatively rare complication of AMI, in particular STE-ACS, in the aggressive coronary reperfusion era, portends worse short-term but not long-term outcomes, and is associated with bigger infarcts in STE-ACS.

Powered by Eventact EMS