
Contemporary Risk Stratification after Myocardial Infarction in the Community: Performance of Scores and Incremental Value of Soluble ST2
2Health Sciences Research, Mayo Clinic
 Background:
Background:
Current AHA/ACC guidelines recommend the GRACE and TIMI scores to assess myocardial infarction (MI) prognosis. Major changes in the epidemiology of MI and the availability of new biomarkers for risk stratification warrant an assessment of the performance of these scores in contemporary practice.
Objectives:
We assessed (a) the performance of GRACE and TIMI to predict 1-year mortality in a community cohort of MI patients stratified by ST- and non-ST-segment elevation MI (STEMI/NSTEMI) and (b) the incremental discriminatory power of soluble ST2, a biomarker emerging as a powerful risk indicator in cardiovascular disease.
Methods: Olmsted County, Minnesota residents with incident MI (N=1,401) were recruited prospectively from 2002-2012 (mean age, 67 years; 61% men; 79% NSTEMI). Baseline data were used to calculate risk scores; sST2 was measured in stored plasma samples obtained at index MI. C-statistics adapted to survival data were used to assess the discriminatory power of GRACE and TIMI score and the improvement gained by adding variables, in particular sST2.
Results:
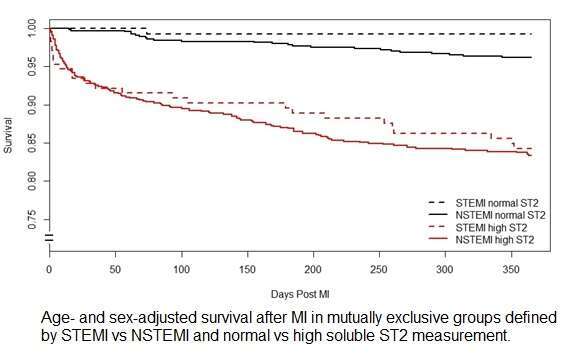
During the first year of follow-up, 190 (14%) patients died. The discriminatory performance to predict death was reasonable for GRACE and poor for TIMI, and was generally worse in NSTEMI vs STEMI. sST2 was a strong predictor of 1-year mortality post-MI, whereas STEMI/NSTEMI status was far less predictive of survival (Figure). In NSTEMI, sequential addition of comorbidities and sST2 substantially improved the C-statistic over GRACE (from 0.78 to 0.80 to 0.84) and TIMI (from 0.61 to 0.73 to 0.81), respectively (all P ≤ 0.05).
Conclusions:
Guidelines-recommended scores for risk assessment post-MI underperform in contemporary community patients, particularly NSTEMI, which now represent the majority of infarcts. Incorporating comorbidities and sST2 substantially improves risk prediction thereby delineating opportunities to improve clinical care.

Powered by Eventact EMS