
Does Compensatory Tricuspid Valve Leaflet Enlargement Prevent Tricuspid Regurgitation in Patients With Pulmonary Hypertension? A 3-Dimensional Echocardiographic Study
2Faculty of Medicine, Technion - Israel Institute of Technology
3Cardiac, Thoracic and Vascular Sciences, University of Padova
Objective:
To determine whether the tricuspid valve (TV) leaflets enlarge in patients with pulmonary hypertension (PH) as a possible compensatory mechanism that may prevent secondary tricuspid regurgitation (TR).
Methods:
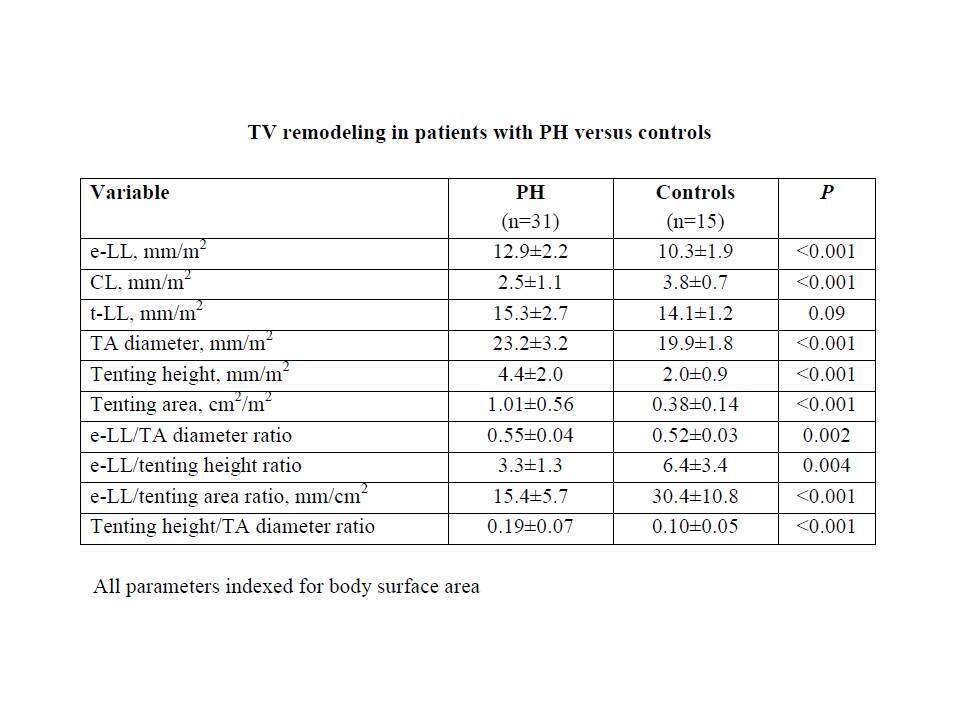
Thirty-one patients with pre-capillary PH (TR pressure gradient 74±23 mmHg) and 15 age and sex-matched controls underwent 3-dimensional (3D) transthoracic echocardiography of the TV (Vivid E9, GE Medical Systems, Horten, Norway). Using 3D-derived multi-plane reconstruction (“Flexi-slice” function) the TV was imaged in 3 planes, each plane dissecting the middle of a TV leaflet and the center of the TV. Effective leaflet length (e-LL, distance from posterior coaptation point to annulus hinge point), coaptation length (CL, distance between leaflet tip and posterior coaptation point), total leaflet length (t-LL = e-LL + CL), tricuspid annulus (TA) diameter, tenting height, and tenting area were measured in each plane and averaged for the 3 leaflets. TR severity was assessed in patients with PH by the proximal isovelocity surface area method.
Results:
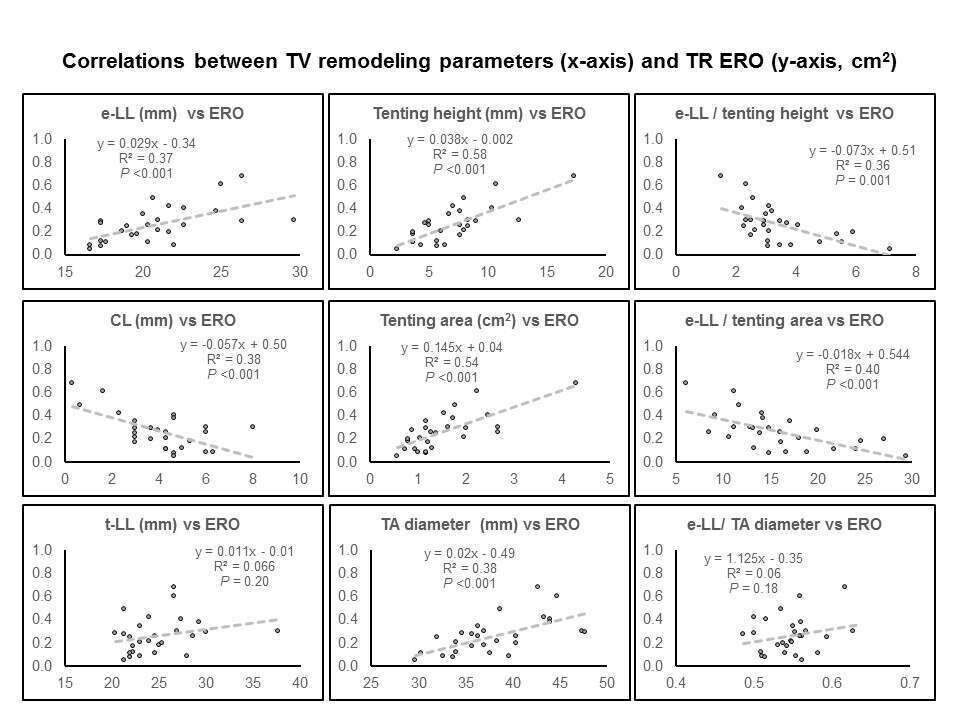
Compared to controls, e-LL increased and CL decreased in PH, with a minor non-significant difference in t-LL (Table). Leaflet tethering was pronounced in PH, to a greater degree than TA dilatation (increased tenting height/TA ratio). e-LL compensated for TA dilatation (preserved e-LL/TA ratio), but not for leaflet tethering (decreased e-LL/tenting height and tenting area ratios). TR severity (effective regurgitant orifice, ERO) correlated positively with e-LL, leaflet tethering, and TA dilatation and negatively with residual leaflet coaptation (Figure). TR was not related to t-LL.
Conclusions:
PH results in pronounced leaflet tethering, TA dilatation, and an increase in e-LL on account of CL, without a significant increase in t-LL. These remodeling processes are associated with the susceptibility to develop secondary TR. Our findings do not support the hypothesis that TV leaflets enlarge in PH as a compensatory mechanism that may prevent TR.

Powered by Eventact EMS