
Tricuspid Valve Remodeling in Pressure versus Volume Overload and its Relationship with Tricuspid Regurgitation Severity: A 3-Dimensional Echocardiographic Study
2Faculty of Medicine, Technion - Israel Institute of Technology
3Cardiac, Thoracic and Vascular Sciences, University of Padova
Objective:
To compare the extent of tricuspid valve (TV) remodeling in patients with pressure versus volume overload [pulmonary hypertension (PH) versus severe pulmonary regurgitation in operated tetralogy of Fallot (TOF)] and the relationship of TV remodeling with tricuspid regurgitation (TR) severity.
Methods:
Thirty-one patients with pre-capillary PH (TR pressure gradient 74±23 mmHg) and 23 patients with operated TOF underwent 3-dimensional (3D) transthoracic echocardiography of the right heart (Vivid E9, GE Medical Systems, Horten, Norway). Using 3D-derived multi-plane reconstruction (“Flexi-slice” function) the TV was imaged in 3 planes, each plane dissecting the middle of a TV leaflet and the center of the TV. Effective leaflet length (e-LL, distance from posterior coaptation point to annulus hinge point), coaptation length (CL, distance between leaflet tip and posterior coaptation point), total leaflet length (t-LL = e-LL + CL), tricuspid annulus (TA) diameter, tenting height, and tenting area were measured in each plane and averaged for the 3 leaflets. Right ventricular (RV) and right atrial (RA) volumes were measured by 3D echocardiography. TR was assessed quantitatively by the proximal isovelocity surface area method.
Results:
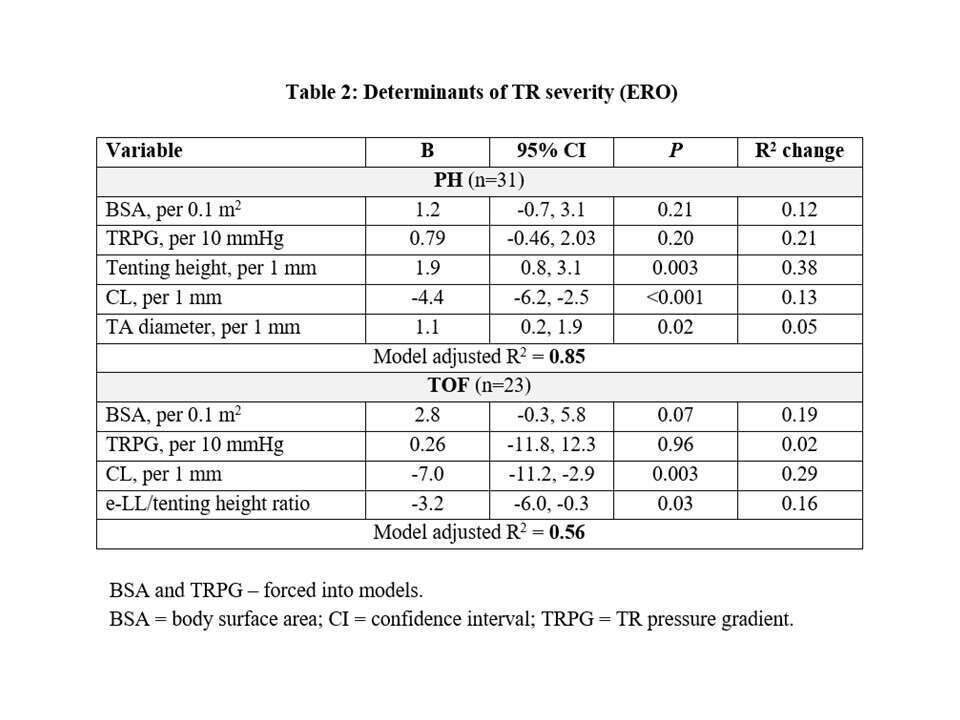
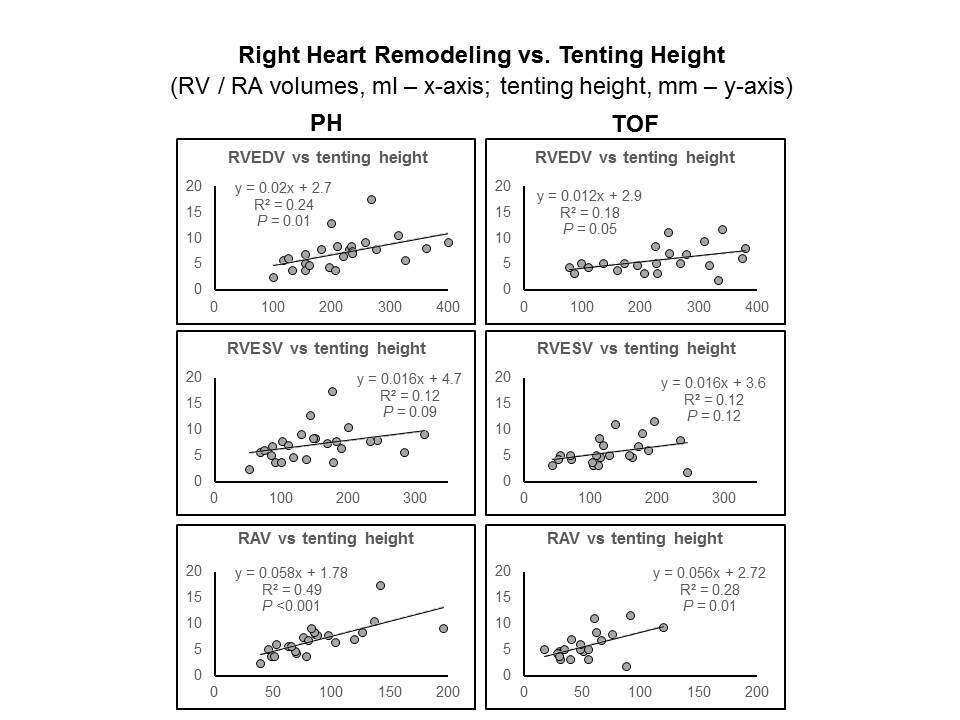
Significant TR was more frequent in PH than in TOF [> moderate TR in 17 (55%) versus 3 patients (13%), respectively, P <0.001]. TV remodeling was more prominent in PH, mainly measures of leaflet tethering (Table 1). By multi-variable linear regression, TV remodeling variables were strongly associated with TR severity (effective regurgitant orifice, ERO) in both groups (Table 2), more so in PH (larger model R2). RV end-diastolic volumes (but not end-systolic volumes or ejection fraction) and RA end-systolic volumes correlated with TV tethering (Figure).
Conclusions:
RV pressure results in significant right-heart and TV remodeling and, eventually, TR. These processes are less pronounced in RV volume overload, thereby explaining the lower frequency of significant TR in RV volume (versus pressure) overload.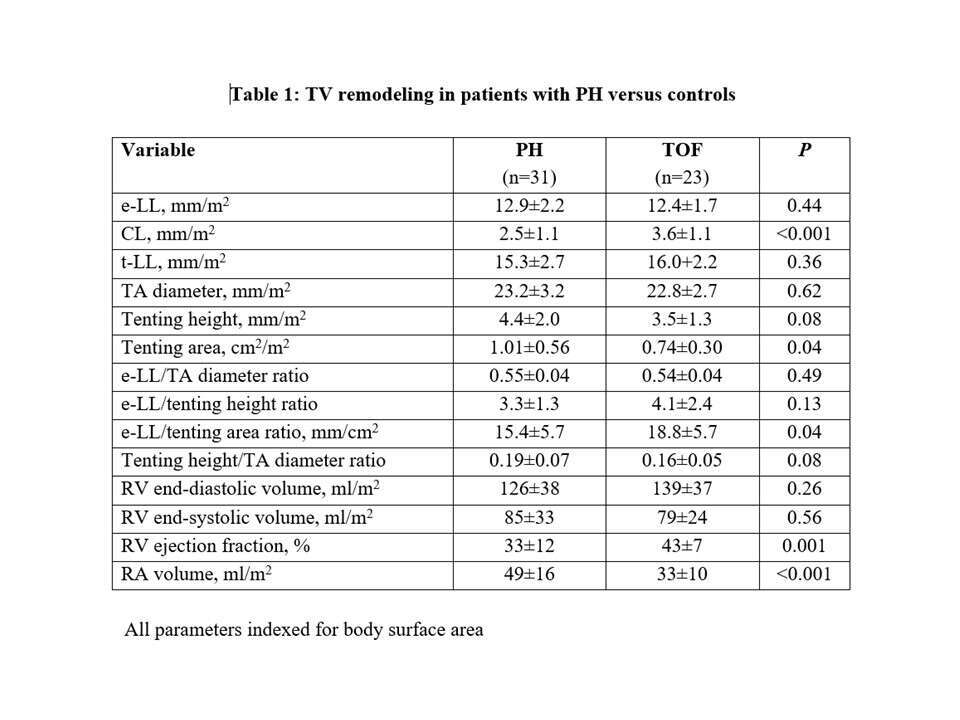

Powered by Eventact EMS