
Death with an Implantable Cardioverter Defibrillator. A MADIT II Sub Study
2Heart Research Follow-up Program, Rochester University Medical Center
3The Sacker Faculty of Medicine, Tel Aviv University
Background and aims:
Data regarding the risk of arrhythmic vs. non-arrhythmic mortality among ICD recipients are limited. We aimed to assess the rate of arrhythmic mortality in ICD recipients who were enrolled in MADIT-II, and to identify factors associated with non-arrhythmic mortality using interrogation data at the time of death during the trial.
Methods:
Patients from the ICD-treatment arm from the MADIT-II trial (N=746) were included. Sixty-eight patients (62% of all deaths) died from cardiac causes with an active ICD. Interrogation data were available for analysis in 44 patients (65%). Arrhythmic and non-arrhythmic deaths were categorized by the presence of ventricular tachycardia or fibrillation (VT/VF) during the terminal event. Multivariate analysis was utilized to find predictors for arrhythmic and non-arrhythmic death.
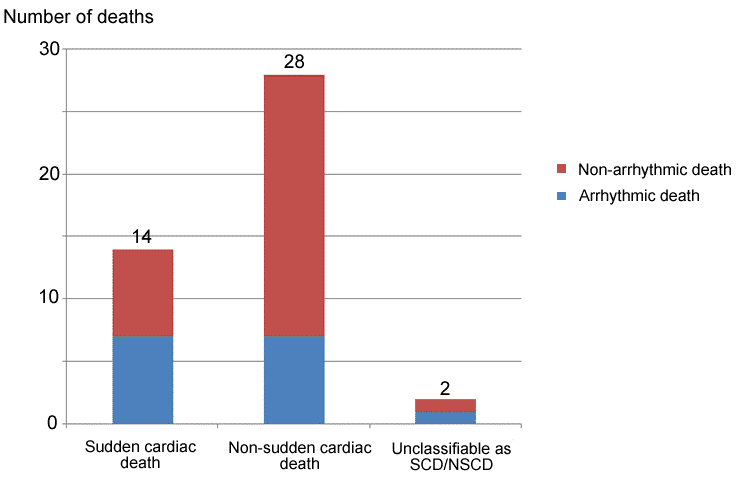
Results:
Fifteen patients (27%) died from arrhythmic causes despite appropriate shocks from the ICD. Only 47% of these deaths were categorized as SCD, while 34% of mortality cases classified as non-sudden were identified as arrhythmic events (Figure). In multivariate analysis, we found that factors associated with non-arrhythmic mortality included: NYHA functional class ≤ II (HR 0.33, p=0.03), lack of history of hypertension (HR 0.25, p=0.03), creatinine < 1.4 mg/dL (HR 0.33, p=0.03), and no prior hospitalization for heart failure (HR 0.11, p<0.01). Previous repetitive shocks for VT of VF occurring more than 72 hours prior to the terminal event were highly predictive for future death from arrhythmia despite appropriate ICD therapy.
Conclusions:
Our findings indicate that current classification of sudden vs. non-sudden mortality fails to identify arrhythmic events at the time of death in a significant proportion of patients, and suggest that patients with ischemic cardiomyopathy who have more advanced heart failure symptoms die from non-arrhythmic causes following ICD implantation.

Powered by Eventact EMS