
Cardiac Troponin Levels to Predict the Risk of Escalation and Mortality in Patients with Pulmonary Emboli
2Non Invasive Cardiology Unit, Sheba Medical Center
3Radiology Department, Sheba Medical Center
Background:
The intermediate risk pulmonary emboli (PE) class gathers diverse set of patients and can carry a significant chronic disability.
Troponin elevation was shown to be an important and independent prognostic factors in patients presenting with acute PE signifying loading of the right ventricle. Accordingly, troponin elevation ("positive troponin") is routinely determined in patients with PE. Nevertheless, the prognostic significance of troponin levels has never been studied. The aim of this study is to determine whether troponin levels carry prognostic significance as in patients with ACS.
Methods:
We evaluated 177 consecutive PE patients categorized as intermediate risk who were admitted between the years 2008-2015. PE was diagnosed based on CT findings. Intermediate risk was determined based on the presence of positive troponin and\or evidence of RV involvement upon either CT or echocardiography.
Patients were stratified according to troponin levels into to tertiles – 0 till 0.12 (ng/L) (T1), 0.12 till 0.70 (ng/L) (T2) and above 0.70 (ng/L) (T3). The primary end-point was a combined end point of mortality (30-days) and the need for escalation therapy during hospitalization (mechanical ventilation, the need for hemodynamic support by inotropes, or the need for secondary reperfusion by either thrombolysis or surgery).
Results:
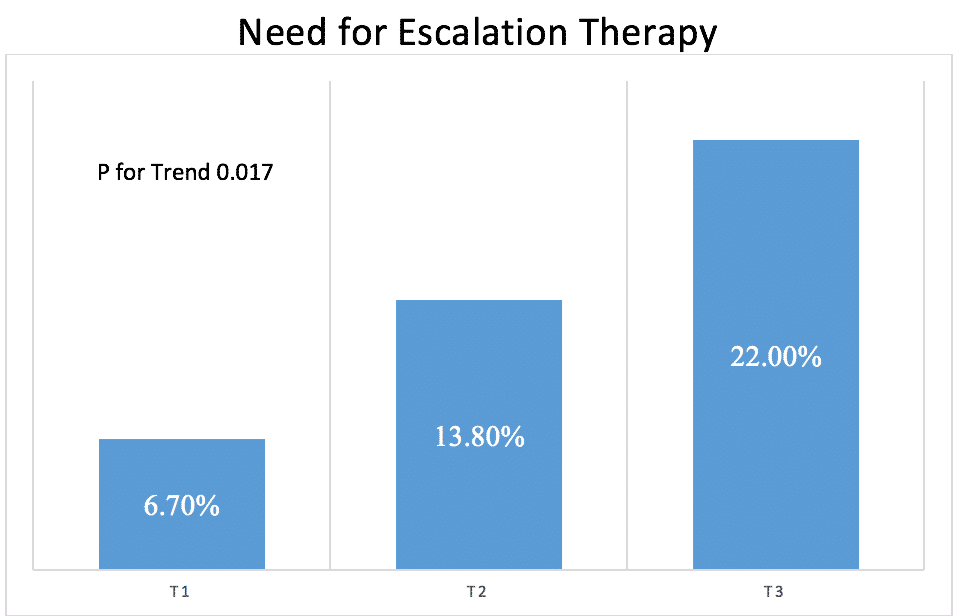
There were no statistically significant differences between the tertiles in regard to baseline characteristics. The occurrence of the primary end-point increased gradually and significantly throughout the tertiles of troponin (6.7%, 14.0%, and 22.4%, p for trend 0.015). This was also apparent for the need for escalation therapy (6.7%, 13.8% and 22.0%, p for trend 0.017) (figure). Thirty-day mortality was higher at T3 (0%, 0% and 5.1%, p for trend 0.033).
Conclusions:
In intermediate risk PE patients, beyond the known prognostic significance of positive troponin level, increasing levels are related to increasing need for escalation therapy and mortality.
Figure

Powered by Eventact EMS