
The Electrocardiographic Frontal QRS-T Angle is a Powerful Predictor of Increased Mortality in Patients with Cardiac AL Amyloidosis
Introduction: Cardiac involvement is a leading cause of morbidity and mortality in primary light chain (AL) amyloidosis. The electrocardiographic spatial QRS-T angle reflects changes in the direction of the repolarization sequence and is a powerful predictor of outcome in patients with heart failure. We examined the significance of the frontal QRS-T angle in predicting the clinical outcome in patients with cardiac AL amyloidosis.
Methods: Forty-three consecutive patients with cardiac involvement of AL amyloidosis were studied. Patient`s charts, laboratory data, electrocardiograms and echocardiograms were reviewed. The QRS-T angle was calculated from the frontal QRS and T axis of the baseline 12-lead surface electrocardiogram.
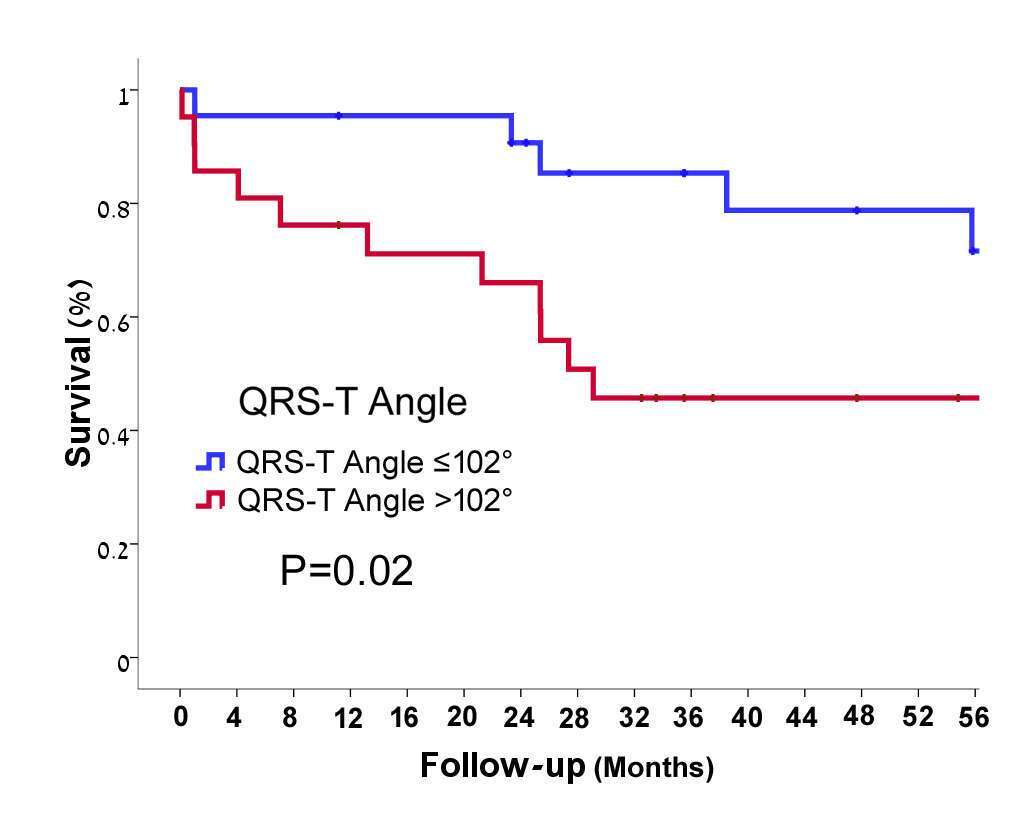
Results: Patients median age was 59.93 years, 55.8% were males. After a median follow up of 32 months (1-133), 16 out of 43 patients had died (37.2%). The median QRS-T angle was 102° (interquartile range 35-148). A QRS-T angle>102° was a significant predictor of increased mortality by Kaplan Meir survival analysis (71.6±11.1% vs. 45.7±11.1%, P=0.02; Figure 1). A QRS-T angle>102° was an independent predictor of increased mortality by Cox regression analysis (hazard ratio (HR) 5.36 (95% CI 1.48-19.34, P=0.01) after adjustment for age, gender, NYHA class and electrocardiographic QRS-pseudo-infarction pattern. QRS-T angle>102° was associated with increased prevalence of Lambda free light chain disease (a more severe disease) and the presence of a pleural effusion. It was also associated with increased LV septal wall thickness, smaller LV end diastolic diameter, echocardiographic myocardial sparkling texture, pericardial effusion, elevated NT-Pro-BNP and evidence of increased restrictive physiology evident by increased E/A and E/e`.
Conclusions: The QRS-T angle is associated with indices of advanced amyloid disease and is a powerful independent predictor of outcome, improving the risk assessment of patients with amyloidosis.

Powered by Eventact EMS