
MyoK+ardial infarction: Changes in K+ Levels are Associated with In-hospital Mortality of Acute Myocardial Infarction Patients. Soroka Acute Myocardial Infarction II (SAMI-II) project
2Cardiology Department, Soroka University Medical Center & Faculty of Health Sciences, Ben-Gurion University of the Negev
3Soroka University Medical Center, Faculty of Health Sciences, Ben-Gurion University of the Negev
Background: Serum potassium levels (K, mEq/L) are associated with outcomes in AMI setting. While significant K levels (KL) changes during AMI hospitalization were reported, their prognostic significance has not been investigated.
Aims: To evaluate the association between fluctuations in K, peak and nadir KL and timing on in-hospital mortality of AMI patients.
Methods: AMI patients hospitalized in a Soroka University Medical Center, through 2002-2012, were studied. Excluded patients: on chronic dialysis, mechanical ventilation, length of stay >3 days or those who underwent emergency coronary-artery bypass-graft. Based on KL during hospitalization, minimal, maximal, and fluctuation (delta between two consecutive KL) were recorded and the associations with in-hospital mortality were assessed using Generalized Estimating Equations model, adjusted to baseline patients’ characteristics.
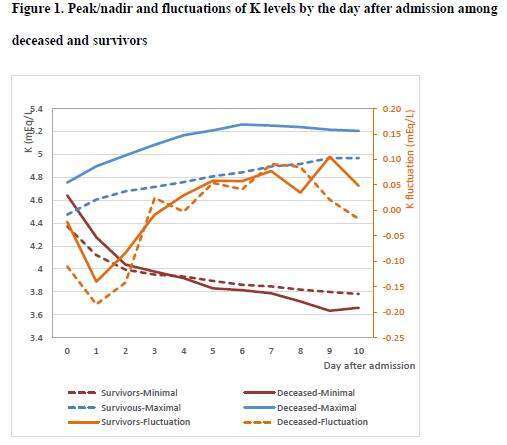
Results: Out of 17,780 admissions (12,535 patients), 13,684 (10,032 patients) were included. In-hospital mortality was 3.7%. KL in the extreme categories were more common among deceased than survivors (P<0.001). Absolute Fluctuations >0.4 mEq/L were more common among deceased than survivors (P>0.001). KL decreased during the first 2-3 days followed by stabilization and tended to be lower among survivors. Minimal and maximal KL were independently associated with increased mortality when moved (either up or down) further from mid- reference range (4.1-4.4) P<0.001 with a “dose response” (e.g. when minimal K<3.8 and maximal K>4.7, OR=34.4, P<0.001). In a multivariate analysis (adjusted for age, comorbidities and blood chemistry), significant absolute fluctuations in K (>0.1-0.4), when resulted in K≥4.4 or ≤3.8, were associated with increased mortality. Cases in which minimal KL was found after the first two days of admission were associated with increased risk for mortality (OR=2.470, P<0.001).
Conclusions: Fluctuations in KL, peak and nadir KL, and the timing of the latter in AMI patients are independent prognostic markers of in-hospital mortality. Close monitoring of KL and fluctuations during AMI is warranted.

Powered by Eventact EMS