
Long-Term Outcomes of 560 Consecutive Patients Treated with Transcatheter Aortic Valve Implantation and Propensity Score Matched-Analysis of Early Versus New Generation Valves
2"Sackler" School of Medicine, Tel Aviv University
Background:
Transcatheter aortic valve implantation (TAVI) has emerged as a safe and effective treatment for severe aortic stenosis (AS) in patients with high or prohibitive surgical risk, and has been rapidly expanding to include lower risk and younger patients. Nevertheless, long term clinical and echocardiographic data is still lacking.
Methods: Analysis of 560 consecutive patients undergoing TAVI at our institution between November 2008 and November 2016 with a median follow up of 1000 days was carried out. Patients were distinguished by access and treated patient tertiles to evaluate temporal changes in TAVI and long-term outcomes. Propensity-score (PS) matched analysis was preformed to compare the impact of the early and new generation valve systems.
Results:
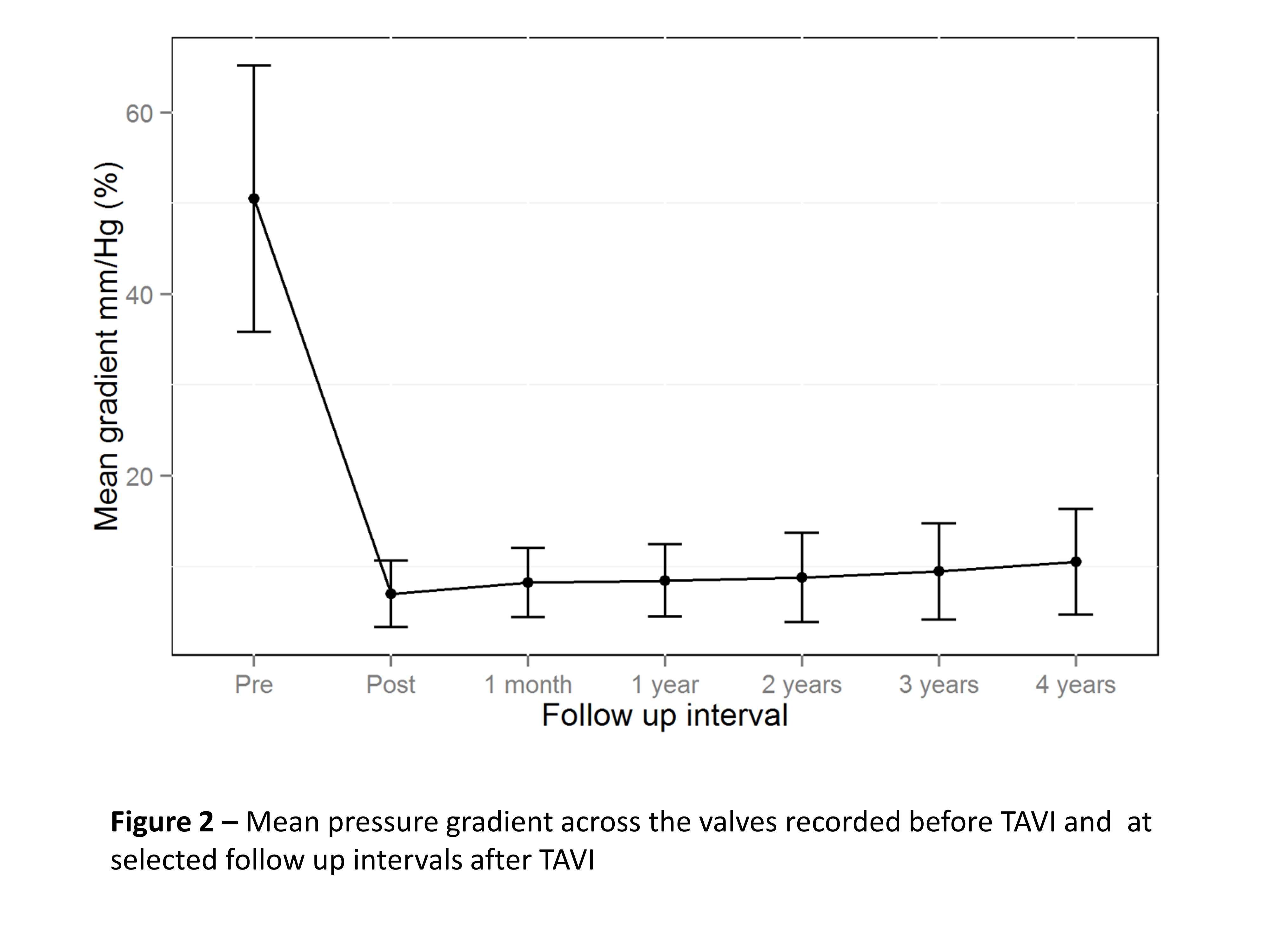
With time, patient selection shifted towards lower risk (mean STS score 8.5 vs. 4.7 in the first and last patient tertile, respectively), and use of conscious sedation and trans-femoral access increased (p mild decreased from 17.5% to 7.6%, p=0.029. Within 5 years 47% of the patients died, most due to non-cardiac causes (72%) [Figure 1]. Independent predictors of 1 year death included periprocedural aspects (vascular complications, stroke and PVL) while death occurring later than 1 year was solely related to untied comorbid conditions (COPD, CKD stage IV/V, Frailty). Transvalvular gradients and residual regurgitation remained favorable up to 5 years follow-up [Figure 2]. New generation valves showed a favorable PVL profile compared to PS matched early generation valves (p=0.05).
Conclusions:
TAVI utilization is expanding to lower risk patients with greater predominance of the transfemoral route. Long term mortality was high and related to population factors rather than to procedural factors. While PVL is effectively addressed by the new generation valves and valve hemodynamics seem durable, efforts to improve long and short term outcomes remains a therapeutic challenge.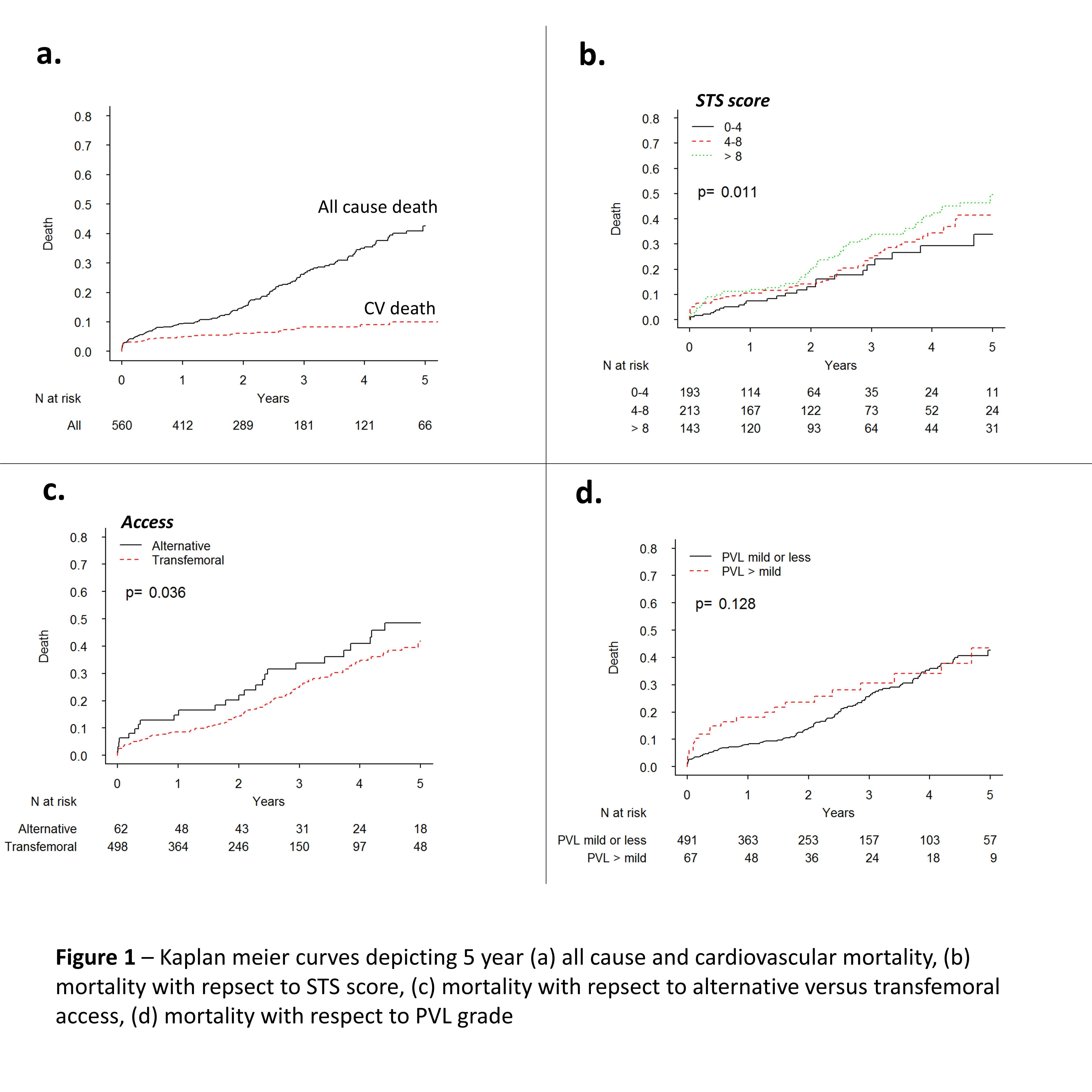
Powered by Eventact EMS