
The Benefit of Implantable Cardioverter Defibrillators in Asymptomatic Patients (NYHA I) with Left Ventricular Dysfunction
2Cardiology Department, Rambam Health Care Campus
3Cardiology Department, Leviev Heart Center, Sheba Medical Center
 Introduction:
Introduction:
Controversy prevails regarding the clinical benefit of primary prevention ICD therapy in asymptomatic patients (NYHA I) with left ventricular dysfunction. We aimed to evaluate ventricular arrhythmia and mortality rates, appropriate device therapies, by NYHA Class in a prospective national ICD registry.
Methods:
The study comprised 1,679 consecutive patients with ischemic cardiomyopathy who were implanted with a primary prevention ICD, and were enrolled in a prospective national Israeli ICD registry from 2010. The risk for clinical and arrhythmic events was assessed by NYHA Class.
Results:
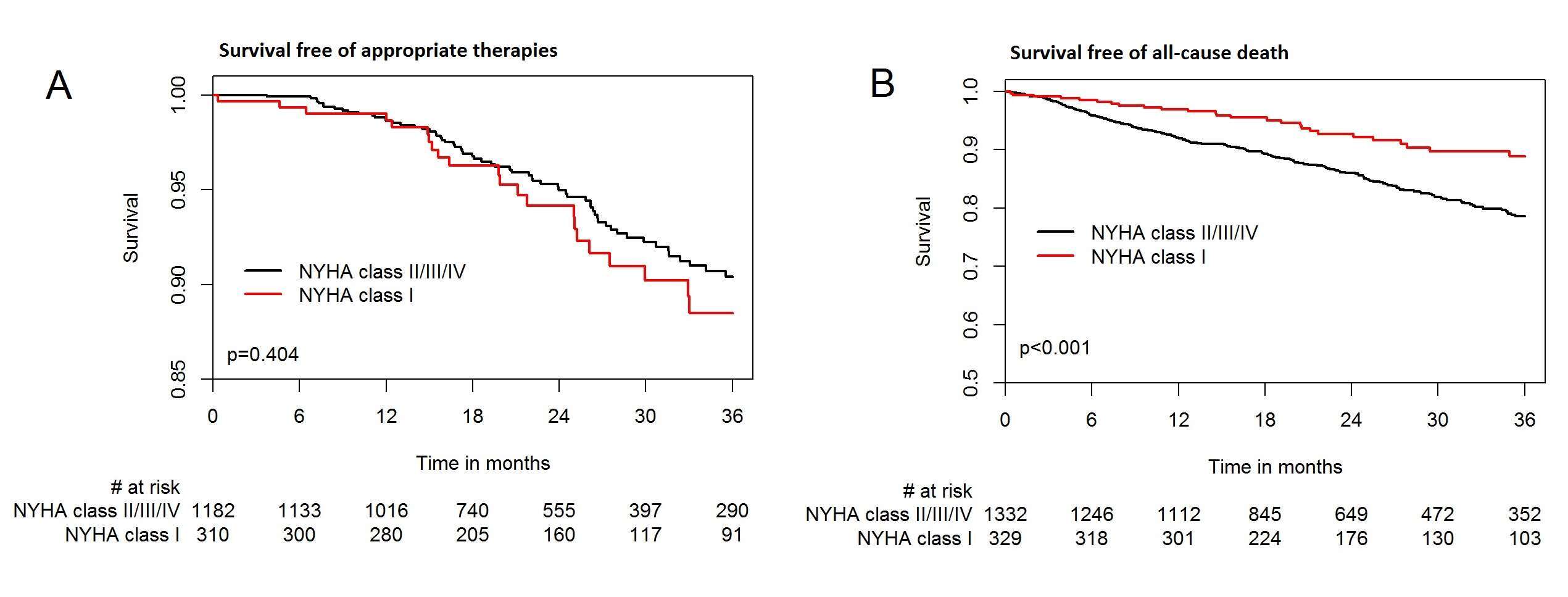
Asymptomatic patients (NYHA I) comprised 20% of the study cohort. -Three year follow-up rates of appropriate ICD therapies were 10% and 12% among patients with NYHA I and NYHA≥II, respectively (p=0.404 [Figure: panel A]). In contrast, mortality rates were significantly higher among the latter group of patients (Figure: panel B). Accordingly, a competing risk analysis between arrhythmic and mortality risk in the two NYHA groups, showed that patients with NYHA I experienced increased likelihood for appropriate device therapy during follow-up after adjustment for mortality risk.
Conclusion:
Our findings indicate that NYHA Class I patients with ischemic cardiomyopathy experience a similar rate of ventricular arrhythmic events and a lower mortality risk compared with symptomatic patients, suggesting that primary ICD implantation may be life-saving in this population.
Evaluate the befit of ICDs in asymptomatic patients with ischemic cardiomyopathy and reduced ejection fraction.

Powered by Eventact EMS