Analysis of Laboratory Samples Rejection for Biotinidase Deficiency (BTD) Screening among Children and Young People in a Mid-Eastern Scottish LA
2Clinical Biochemistry Department, NHS Fife
3Paediatric Neurodevelopmental Service, 1Cambridgeshire and Peterborough NHS Foundation Trust, University of Cambridge Health Teaching NHS Trust
Background: Specimens submitted to the Pathology laboratories are usually rejected as unsuitable for analysis for various reasons at an approximate mean rate of 0.3% and up to 0.75%, but higher values of up to 13% have also been reported. Pre-analytical errors largely related with procedures outside the laboratory are usually the commonest causes of rejection but the majority of them are preventable.
Method: Laboratory and clinical data of all patients screened for BTD over a two-year period across NHS Fife were retrospectively analyzed. All the blood specimens for Biotinidase tests were sent to a central laboratory at Edinburgh for analysis. Research Ethics Committee approval was not required, as this was a retrospective audit using routinely collected anonymised data from the laboratory computer system.
Results: NHS Fife is one of the fourteen regions of NHS Scotland. Fife is a large rural area with a total estimated population of 368,280 (Mid 2015), of which 17.4% are children aged 0 to 15 years old 64081.
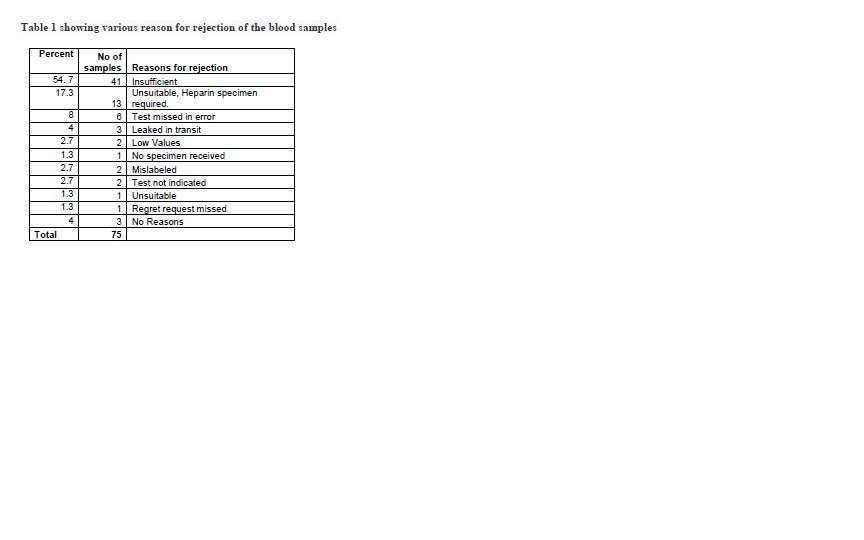
A total of 262 tests (equivalent to 2 per 1000 per year) were requested for 243 children aged between 1 and 153 months (Mean 70 months). 75 samples were ordered to be repeated. 15 patients had their samples repeated once and two patients had their samples tested twice, giving a repeat sampling rate of 19/75 (25%). Various reasons for repeat testing, the commonest being “Insufficient sample” (Table 1). 56 samples from 53 (22%) patients were unsuitable for analysis. None of the 191 patients’ samples analysed had abnormal BTA results.
Conclusion: There is an exceptional high rate of sample rejection and low rates of re-sampling for Biotinidase screening tests, well above the universally reported levels. Further studies are required to better understand the reasons for this observation and to devise strategies to reduce these incidents in the future.

Powered by Eventact EMS