Case Report: Faces of Multiple Respiratory Tract Infections
2Pathological Anatomy Clinic, Department of Cytology, Hospital of Lithuanian University of Health Sciences, Kauno Klinikos
Background: Atypical and combined respiratory infections can present with different clinical symptoms and mimic various diseases. Unfortunately the diagnosis is sometimes difficult and usually retrospective.
Aim: To present case report about complex of various clinical symptoms and rare brochoscopic changes caused by combined respiratory infection.
Methods: Retrospective analysis of the patient‘s medical data.
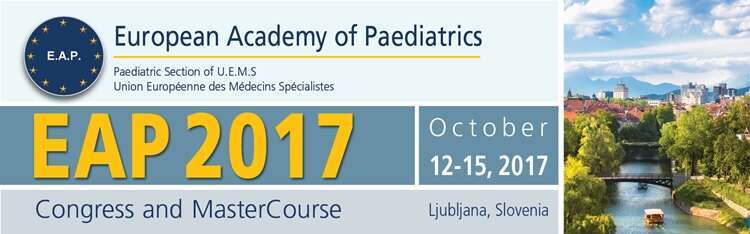
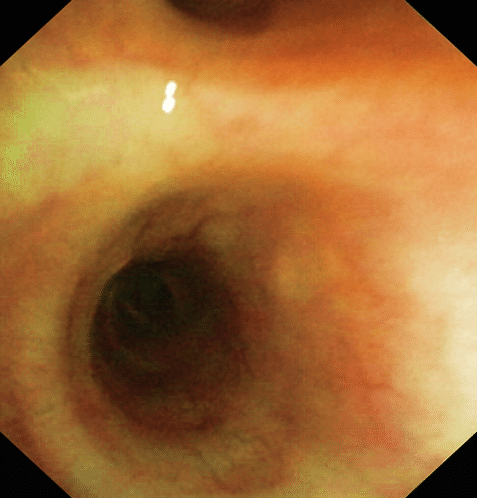
Results: 11 y old boy was admitted to the hospital due to severe hyponatremia, low grade fever, mild diarrhea and cough. Lung auscultation was normal, later crackles on the right side appeared. Chest X-ray showed infiltration on the right, blood test was normal. Suspected pneumonia was treated with Penicillin following with Clarithromycin. On the 9th day changes on the X–ray decreased, IgM Mycoplasma and Chlamydia pneumonia were negative, the boy was free of symptoms therefore he was discharged from the Clinic. Four days later the patient returned back because of high fever, dry cough and moderate diarrhea. Crackles on the right side were detected again, mild bronchial obstruction appeared. However, blood test, Chest X-ray were normal, spirometry showed mild partially reversible bronchial obstruction. Symptomatic treatment was not effective. Bronchoscopy showed infiltration of the right bronchus with soft multifocal nodules (Fig.1) without clear origin. Lymphocytes with some alveolar macrophages (Fig.2) were present in the cytology. Paired sera for Mycoplasma pneumoniae was positive and Boca virus was identified from the nasopharyngeal swab. Azithromycin was given because of persistent respiratory symptoms and confirmed atypical infection. After ten days repeated bronchoscopy was normal (Fig.3), the patient was clear of all symptoms.
Conclusion: Human Boca virus was the leading pathogen of the whole clinical picture in our patient. Co-infection with Mycoplasma pneumonia stimulated more severe and complicated disease. Suspition and identification of possible infection on time is very impotant for further clinical decisions.
Fig.1

Fig.2
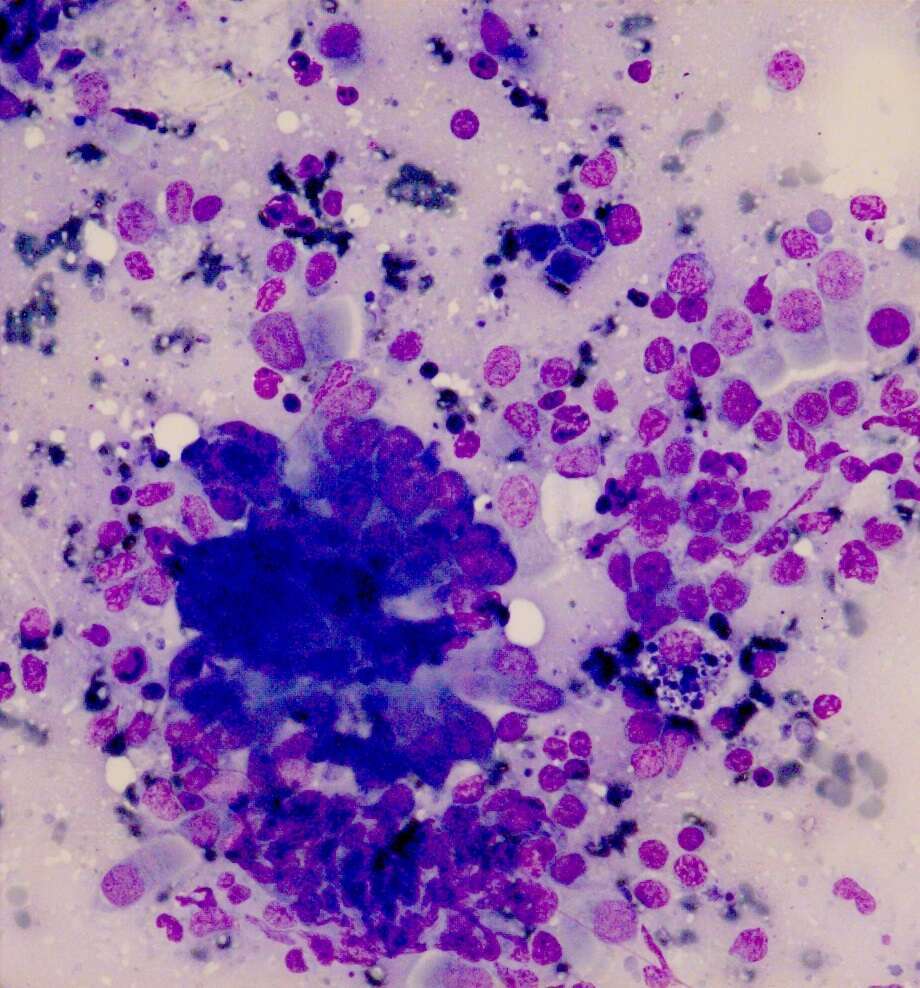
Fig.3

Powered by Eventact EMS