The Where and the Why of Intravenous Antibiotic Treatment for Febrile Urinary Tract Infection/Pyelonephritis in Children
2Clinical Paediatrics, The Murdoch Children's Research Institute
3Paediatrics, Univerisity of Melbourne
4Paediatrics, The Royal College of Physicians of Ireland
Introduction: Febrile UTI/pyelonephritis is a common diagnosis for children presenting to the Emergency Department(ED). A Cochrane review of the management of pyelonephritis in children showed no difference between intravenous(IV) and oral antibiotics. Despite this, many children are treated with at least initial IV antibiotics. The reasons are often unclear and it is uncertain whether this is appropriate as the Cochrane review excluded children at the worse end of the clinical spectrum. Our aim was to determine why physicians made these decisions as a first step in determining whether this is necessary.
Methods: A prospective observational study of children presenting to the ED at the Royal Children’s Hospital with UTI/pyelonephritis from Oct.2016-Apr.2017. Data collection included demographic, clinical features, microbiology, treatment and outcomes. ED physicians were asked to record reasons for prescribing IV antibiotics and for treating the patient in hospital versus in hospital-in-the-home(HITH).
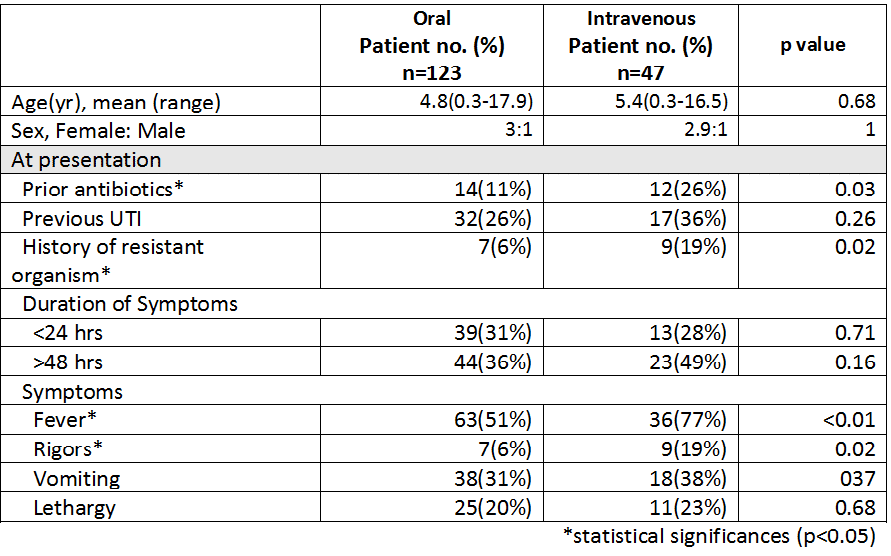
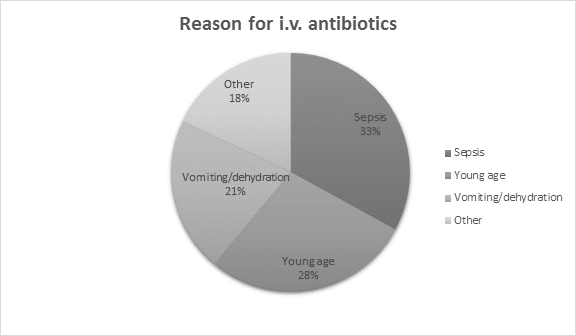
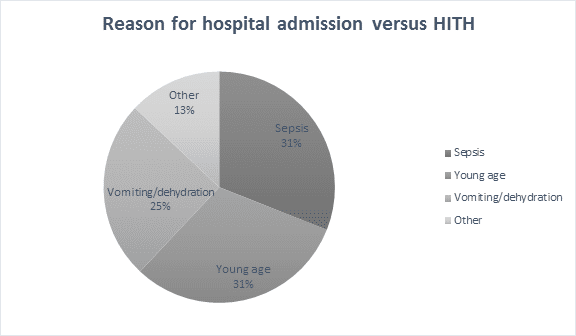
Results: 170 children were included, 123(72%) were treated with oral antibiotics, 43(25%) IV and 4(3%) intramuscular – these are now included in the IV group. In the IV group, 32(19%) were admitted, 3(2%) were transferred directly to HITH from ED and 13 had a single dose of IV antibiotics in ED and were discharged. A comparison of clinical features between the two groups is outlined in the table. The commonest reasons cited for using IV antibiotics and for hospital admission versus HITH are shown in the figures.
Conclusions: This is the first study of decision-making for IV antibiotics and hospital admission for UTI/pyelonephritis in children. The fact that the reasons cited for IV antibiotics were often not evident on objective clinical data suggests that there may be overuse of IV antibiotics. We will present an assessment of appropriateness and use the results to suggest alternatives to the traditional IV and hospital admission route for these children.

Powered by Eventact EMS