focused Optimal Coronary Ultra Sonography (focus): A Novel Methodology for Coronary Image Evaluation in Acute Kawasaki Disease
Background: Acute Kawasaki Disease(KD) may induce coronary artery abnormalities (CAA) in 25-40% of the patients based on published document. Golden diagnostic criteria of acute KD with CAA requires diameter Z score>2.5 along with perivascular brightness and lack of tapering. However, the systematic evaluation of these parameter is uncertain.
Objective: To develop a thorough scoring system useful in systematic evaluation of coronary arteries lesion.
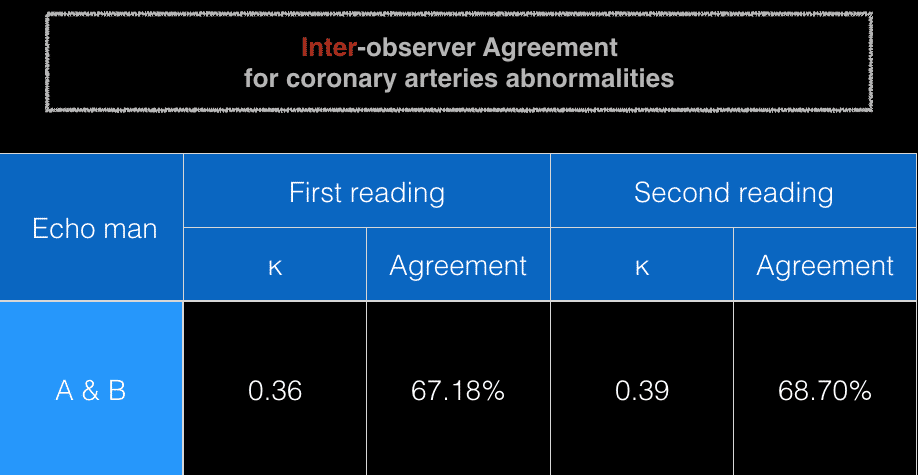
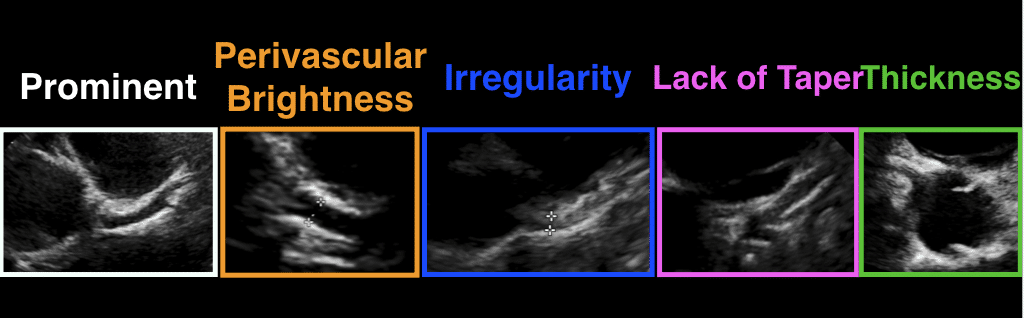
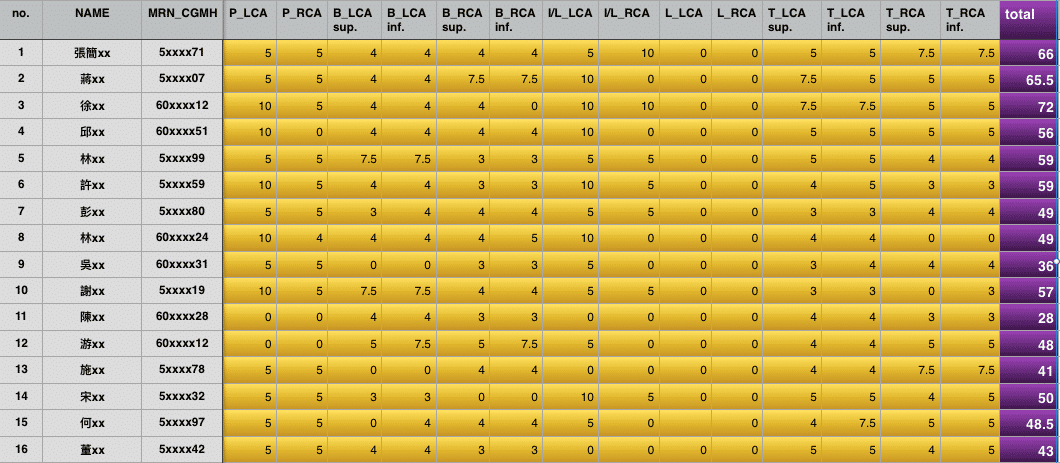
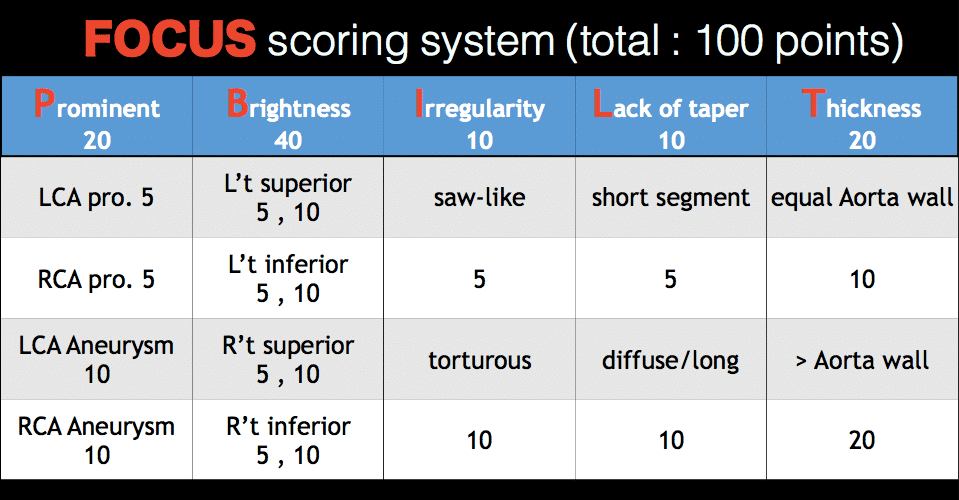
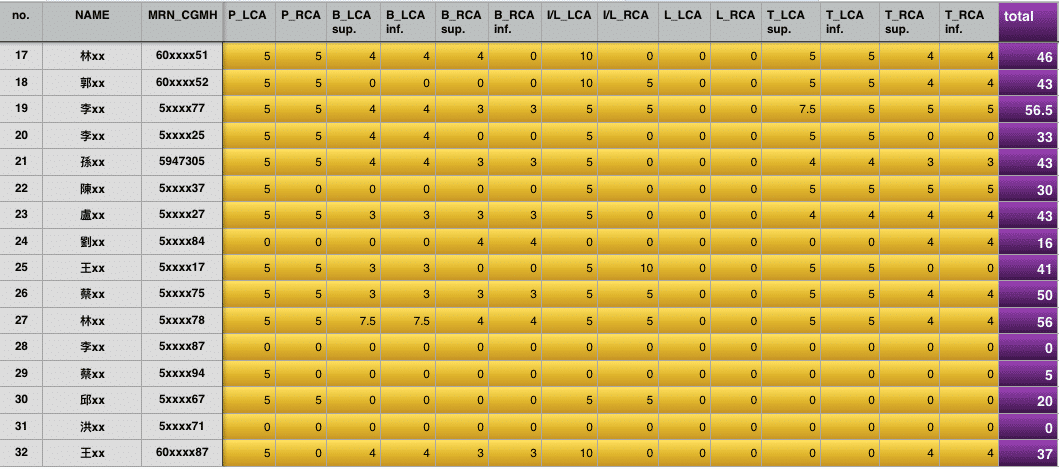
Methods: 32 children with acute KD plus 100 age-match normal children were assigned to 2 experienced cardiologists who wasn’t informed the diagnosis for echocardiography (echo) performed by obtaining dynamic cine-loop recording for frame-by-frame analysis and using quality-optimal highest transducer frequency. CAA are scored as following: 1) Prominence 2) Brightness of arterial wall 3) Irregularity arterial lumen or Lack of tapering 4) Thickness of the arterial wall. Weighted kappa statistics were used to analyze inter-observer and intra-observer agreement, and the agreement percentages were calculated
Results: Various CAA were present in acute KD, include various degree of luminal prominence in 24 (75%) patients, aneurysm formation in 3(0.9%) patients, lack of tapering in 22(68%) patients, irregularity in 11(34%), and intimal thickening brightness in 24 (75%) patients. Overall, coronary artery anomalies were present in 30 (93%) of our patients in acute phase of KD. FOCUS score >10 in 90.6% (29/32) of patients while only 0.6% (2/32) FOCUS score
Conclusion: The incidence of coronary artery abnormalities in acute KD is higher than previously reported. With our novel FOCUS scoring method, more detailed, comprehensive and multi-faced features of CAA other than conventional Z score can be provided. We thus propose a FOCUS score >10 is indicative for acute KD,

Powered by Eventact EMS