
Requiem for; Ones ICU from ED-wards, Twice ICU to Grave-yards
Background: ICU prognostic scoring systems usually don’t conclude just depending on patients’ “from-where” condition, or, even though some included it in, but not with a high coefficient, indeed. However, ICU Patients admitted directly from ED were usually sensed to have worse prognosis.
Objective: We assessed the hypothesis of that; ICU patients from ED have not worse prognosis then score based prediction.
Methods: Retrospective data of mixed-type ICU, in 2016, were assessed for admission types and mortality rates. Diagnosis-weighted predicted death rate for APACHE II scores and observed mortality rates, and also between genders, were compared. Diagnosis types were also analyzed for effect by regression analysis, at significance of p.
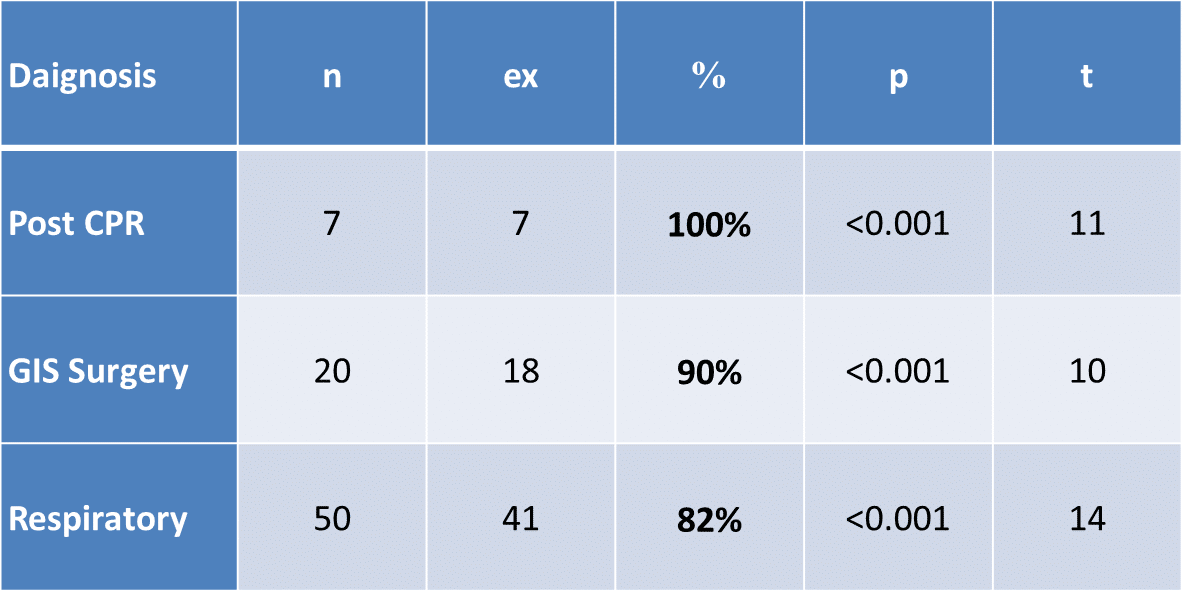
Results: Total of 109 patients out of 347 (31.4%) (m:68, f:41) were admitted directly from ED. Of all 85 ended ex (78%) (m:57, f:28). The mean age was 67.5±7.3 years, APACHE II score 23.4±7.3, LOS 9.1±1.2 days. The mean “diagnosis-weighted predicted death rate for APACHE II scores” was calculated as 41%, on the other hand, observed was 78%, with no gender difference (Table 1). Post-CPR patients, patients required emergency GIS surgery and respiratory arrests ended with more than 80% mortality (Table 2).
Conclusion: Here it was showed; about 30% of ICU patients were ED origin, and, had twice risk for mortality against predicted-score. Therefore, intensivists should not just rely on score based predictions for ED-ICU patients.
Table 1: Diagnosis-weighted predicted death rate for APACHE II scores and observed mortality rates, and between gender comparisons.
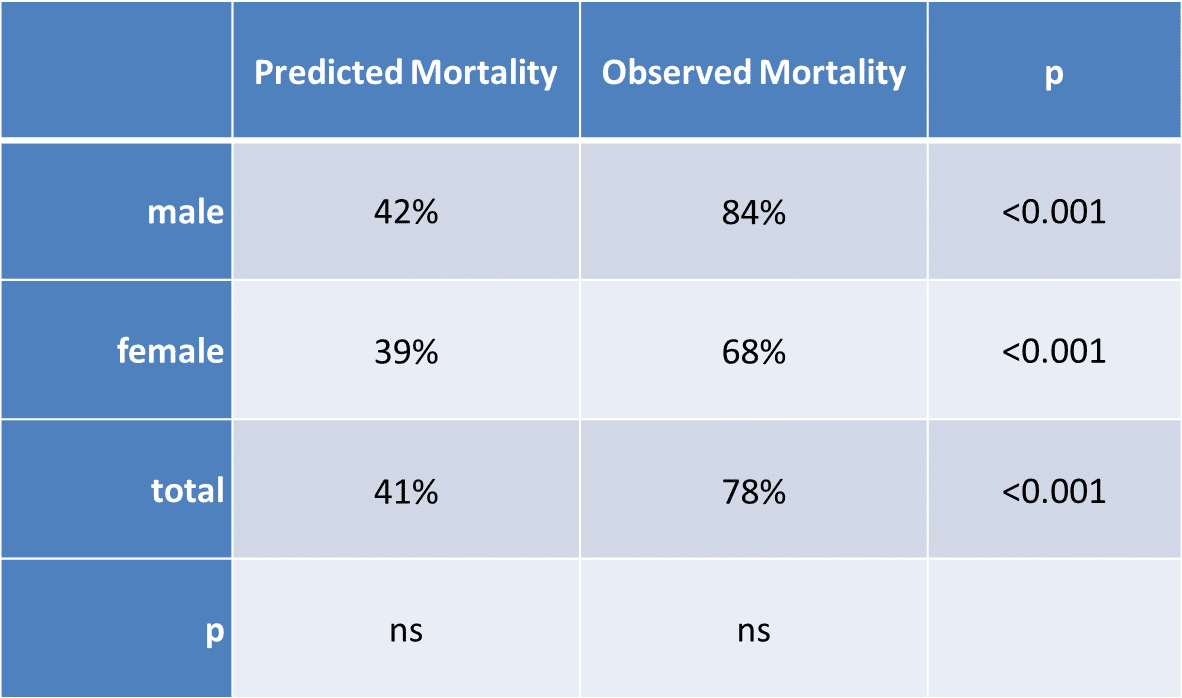
Table 2: Regression analysis of diagnosis factors.
Powered by Eventact EMS