
Coronary Artery Disease Risk and Genetic Risk Score According to Presumed Physiological Function
2Cardiology Department, New University of Lisbon
Recent studies have led to a better understanding of the genetic architecture of coronary artery disease (CAD). It mostly derives from the cumulative effect of multiple common risk alleles, individually with little effect on risk but with considerable effect when combined into specific scores.
Objective: Based on 33 genetic variants associated with CAD or with intermediate phenotypes of traditional risk factors (TRF), we aim to calculate multiplicative genetic risk scores (GRS) according to the presumed physiological functional axes and, subsequently, determine the CAD risk when to number of affected axes.
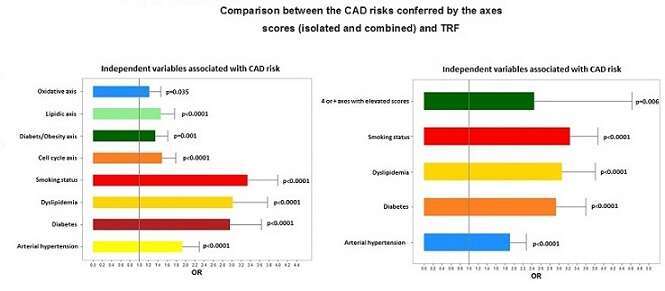
Methods: A case-control study with 2888 subjects was performed, including 1566 consecutive coronary patients and 1322 controls. GRS of 5 major pathophysiological risk axes were calculated: RAAS, Lipids metabolism, Oxidative stress, Diabetes/Obesity, and cell cycle. Comparison of 2 logistic regressions (LR) models was performed: Adjusted model for TRF + 5 GRS and extended model of TRF and number of elevated (>75% percentile for controls) GRS axes.
Results: The cell cycle GRS showed highest CAD risk for (OR=1.49; p<0.0001), followed by the lipid axis with OR=1.46; p<0.0001, diabetes and obesity: OR=1.35; p=0.001 and oxidative axis OR=1.22; p=0.035. The RAAS GRS score did not reach statistical significance. The second LR showed that a higher number of elevated score axes had a significant risk for CAD (OR=2.45; p=0.006).
AUC for adjusted model was 0.738 and improved when adding the 5 axes scores (AUC=0.753) with statistical significance (Delong test, p<0.0001).
Conclusion: The diagnostic and prognostic value of the Total GRS is already well established. In addition, analyzing the GRS by axes we can provide one important direction to better understand the pathogenesis of CAD mainly in the patients without TRF and to develop new and improved preventive measures and new treatments in these important set of patients.

Powered by Eventact EMS