
Progressive Calcification of the Coronary Tree in an Athlete with High Factor VIII
2Cardiología nuclear, Laboratorio de imagen cardimax
A 43-year-old male patient presented an anteroseptal infarction without residual ischemia in 2010 and 2 parieto-temporal infarcts two years later, without neurological deficit nor clinical cardiac failure.
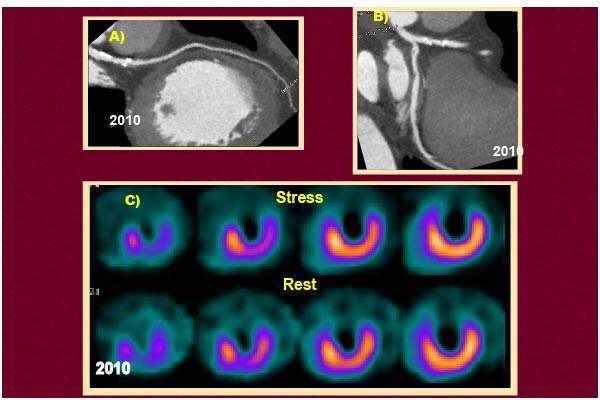
Five years later, a coronary MSCT (Fig.1) showed mild calcification in LDA, however he remained asymptomatic.
In 2017 the patient noticed mild dyspnea during his regular exercise practice, although he requested cardiac evaluation until his dentist planned a gum elective surgery.A stress treadmill test was positive for ischemia. A new SPECT and MSCT were performed and showed mild apical-inferior ischemia, (LVEF: 27% at stress; 37% at rest), plus an extensive amount of calcium along the proximal LAD and Cx. (Fig. 2).
An ICA with 2 stents (LAD and Cx), were successfully placed.
The relation of CAD with acute coronary syndrome and elevated factor VIII is well documented. Atherosclerosis can progress and put the patients’ lives at high risk without regular medical supervision.
The use of SPECT and MSCT modified the natural evolution of the disease: an ICA was possible just because both noninvasive tests were performed; therefore quality and expectancy of life were improved.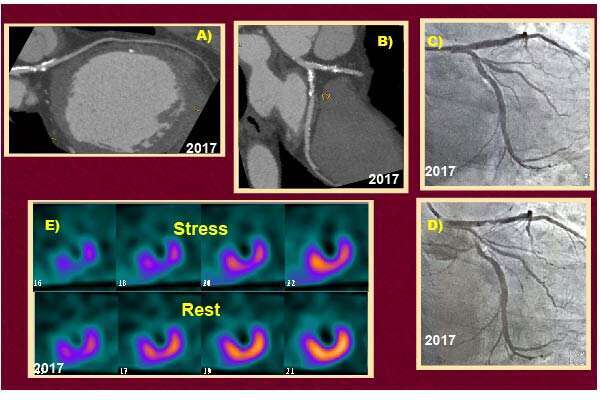
Powered by Eventact EMS