
The Effect of Isolated Weber B Fibular Fracture Displacement on Tibio-Talar Contact Pressures - A Cadaveric Study
2Podiatric Surgery, Columbia St Mary's Hospitals, Milwaukee
3Orthopaedic Surgery, Virginia Commonwealth University School of Medicine, Richmond
Background: Surgical treatment of Weber B fractures without clinically significant talar shift or medial ankle disruption remains controversial. This study measured the contact area and peak pressures of the ankle joint in a cadaveric model with serial displacement of the distal fibula in two isolated Weber B fracture patterns.
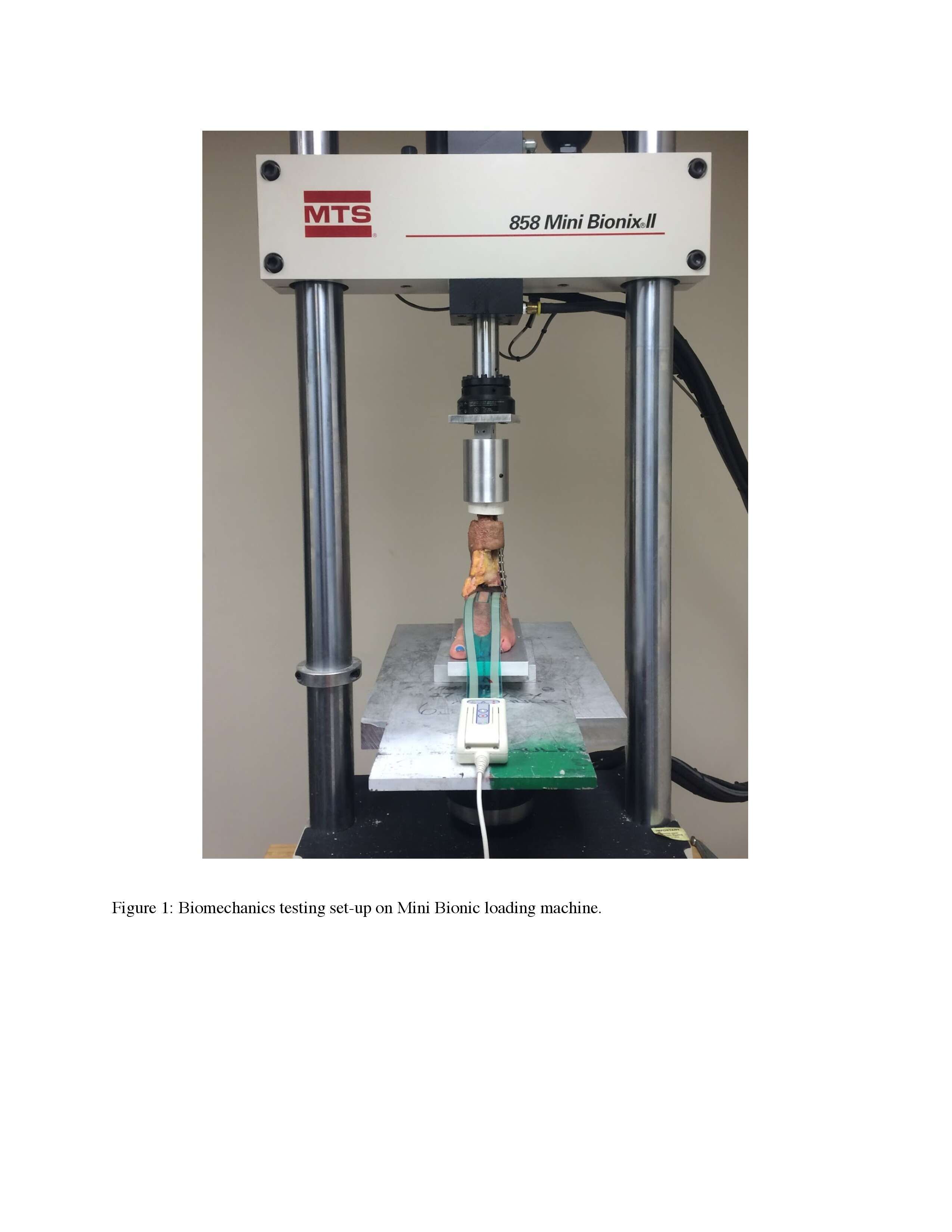
Methods: 6 matched pairs of ankle cadaveric specimens were mounted onto a Mini Bionix (MTS Inc. Eiden Prairie, MN) loading machine and subjected to a 70kg axial compressive load (Fig.1). A Tekscan pressure sensor was placed in the ankle joint to monitor the pressure distribution and contact area. Each specimen was tested at baseline in neutral (Fig.2) and varying degrees of flexion. Transverse (TV) or spiral (SR) Weber B fractures were tested at varying degrees of displacement. Specimens were subjected to the same static, axial load and positions as intact specimens. ANOVA (two-sided, α <0.05) compared the peak pressures and contact areas among intact, TV, and SR specimens.
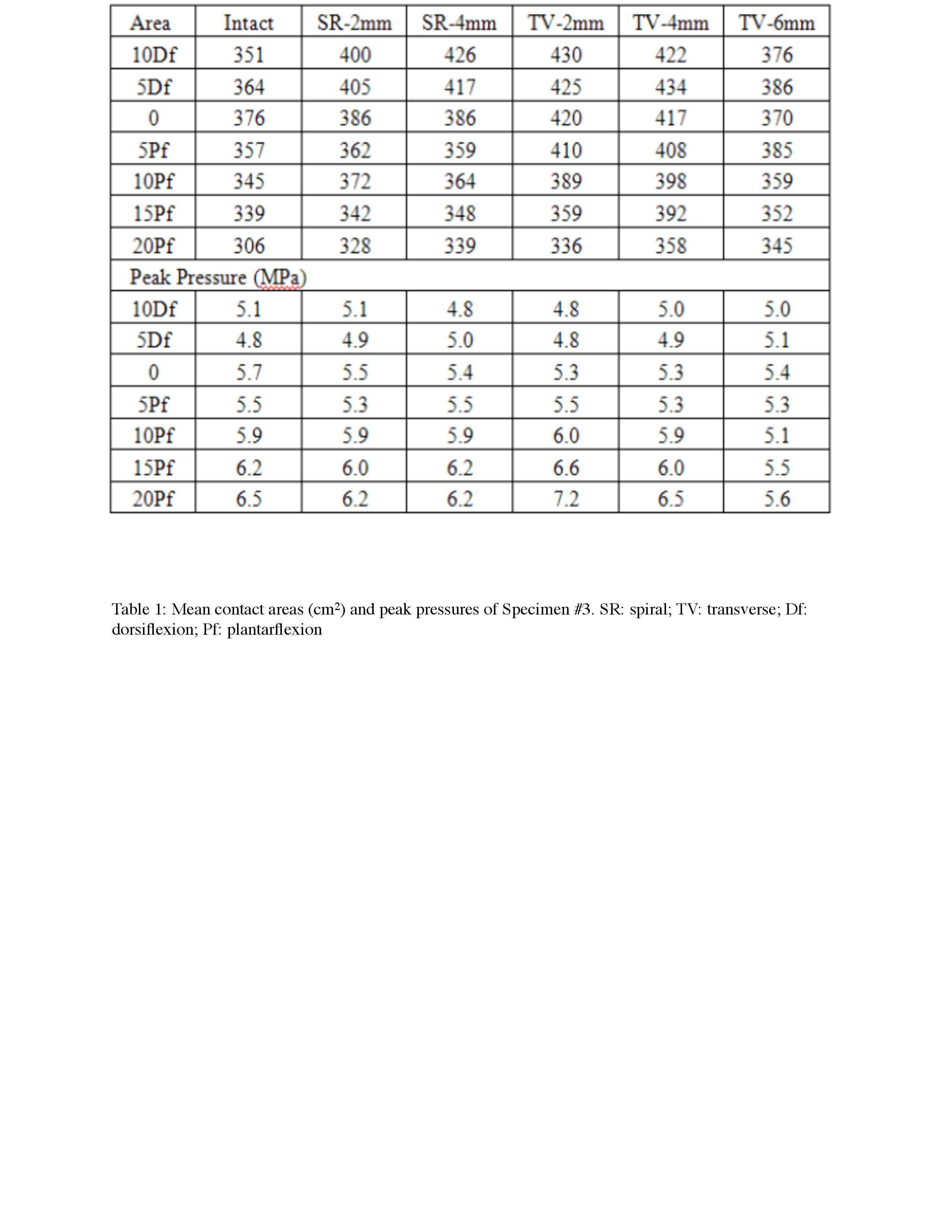
Results: Average contact areas of the intact specimens (376 mm²) was slightly smaller than those of the TV (420, 417, and 370 mm² at 2, 4, and 6mm translation respectively) and SR (386 mm² and 386 mm² at 2 and 4mm translation) specimens, but without statistical significance (Table.1). The average peak pressure of the intact specimens (5.7MPa) was slightly higher than TV (5.3, 5.3, and 5.4MPa at 2, 4, and 6mm translation respectively) and SR (5.5 and 5.4MPa at 2 and 4mm translation) specimens, although not statistically significant.
Conclusions: Isolated Weber B fractures with the distal fibula displaced laterally up to 6mm or superolaterally up to 4mm lateral translation and 10 degrees external rotation do not cause ankle instability. In our model, without significant loss of joint congruence, there is no increased risk of post-traumatic arthritis, therefore mitigating the need for surgery.


Powered by Eventact EMS