
The Trick with the Wire
Background: Endobronchial blocker (EB) placement for thoracic procedures in infants is challenging. Small airways, manipulation in the lateral position, and blocker dislodgment are some of the problems.
Objective: We describe an innovative technique (according to Enk) facilitating placement of the EB.
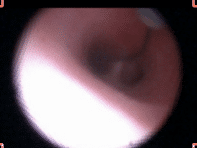
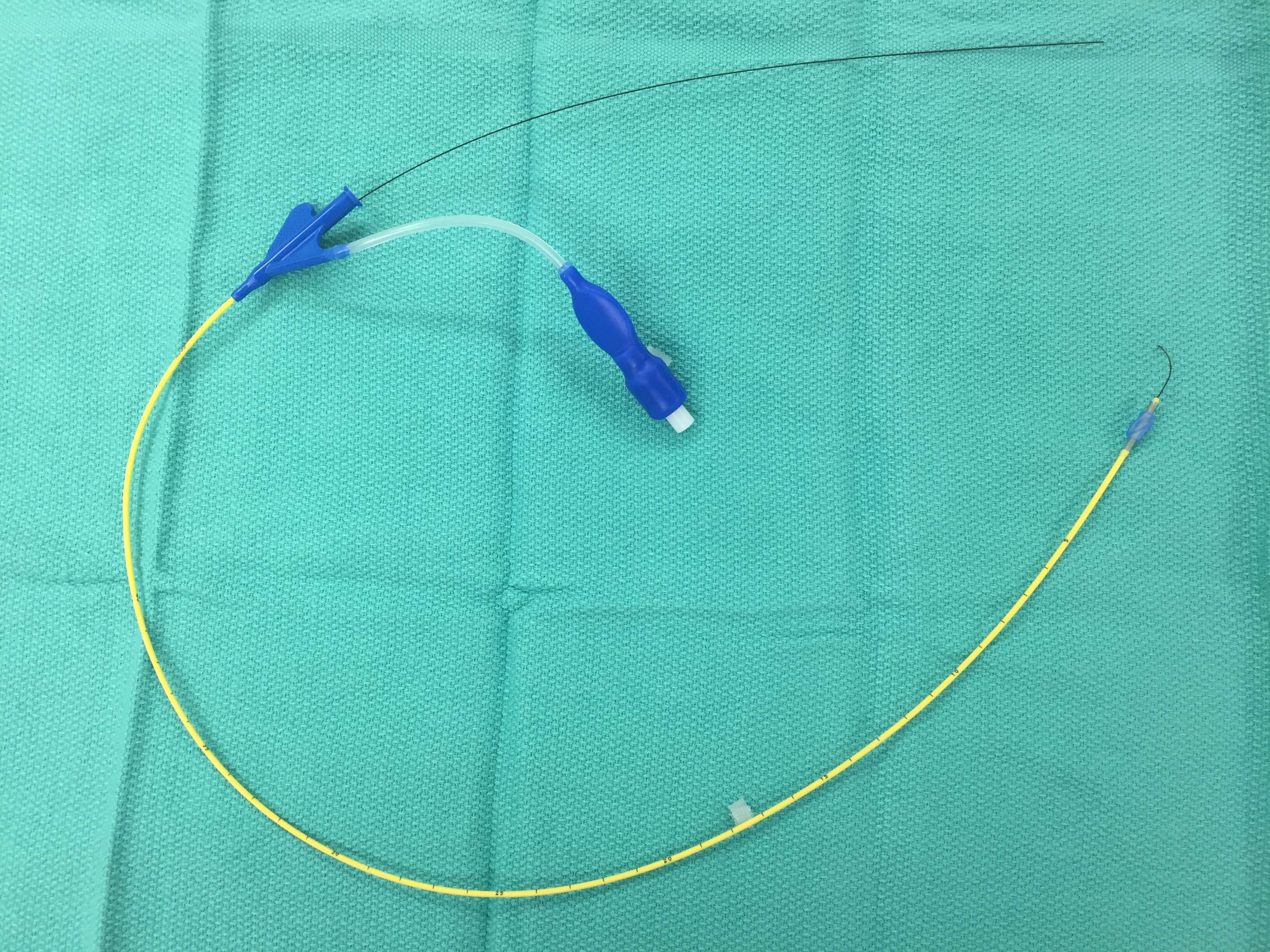
Method: A 5 French EB (blue nylon loop removed) is flushed with saline. A hydrophilic coated wire (0.025inch) with an angled, half-J tip is placed, such that the wire protrudes past the tip of the EB. The wire needs to slide easily. By simply rolling the wire between two fingers the angled tip can be turned right and left. With direct laryngoscopy, the EB (wire pulled back inside) is now placed into the trachea and an appropriately sized endotracheal tube (ETT) introduced beside the blocker. The patient is positioned in the lateral decubitus position. We then place the fiberscope through the ETT to locate the EB. Under vision, we advance the wire beyond the tip of the EB. By twisting the wire at the distal end it is directed into the desired bronchus. Next, we position the EB over the wire and visualize inflation of the cuff. Once the cuff is in the correct position, we secure the EB, and remove the wire to allow lung deflation.
Discussion: We have successfully used this technique in several patients. It minimizes time to place the EB and allows for easy repositioning of the EB if needed. Keeping the wire “loaded” stabilizes the EB and may reduce the risk of dislodgment.

Powered by Eventact EMS