
Pyloric Stenosis: To Rsii or not to Rsii

 Background: RSII has been the preferred induction technique for infants with pyloric stenosis for years. There is a dearth of evidence to support its efficacy in preventing aspiration. Furthermore, it poses specific risks to the pediatric population. Recently, we changed our practice to a “controlled RSII” (cRSII) technique as described by Weiss. This method allows low pressure mask ventilation till intravenous medications provide optimal conditions for intubation. Cricoid pressure is not applied, and depolarizing neuromuscular blocking agents may or may not be used.
Background: RSII has been the preferred induction technique for infants with pyloric stenosis for years. There is a dearth of evidence to support its efficacy in preventing aspiration. Furthermore, it poses specific risks to the pediatric population. Recently, we changed our practice to a “controlled RSII” (cRSII) technique as described by Weiss. This method allows low pressure mask ventilation till intravenous medications provide optimal conditions for intubation. Cricoid pressure is not applied, and depolarizing neuromuscular blocking agents may or may not be used.
Objective: Retrospective review examines the incidence of complications secondary to change in induction technique
Method: A retrospective chart review was conducted for infants presenting for pyloromyotomy June 2010 to September 2015. Data collected included age, gender, weight, surgical and anesthetic induction technique, pre-operative suctioning, muscle relaxants used. Primary outcome parameters were hypoxemia (SpO2 <90%), and regurgitation/aspiration during induction and intubation. Secondary outcome parameter was hypotension (systolic BP
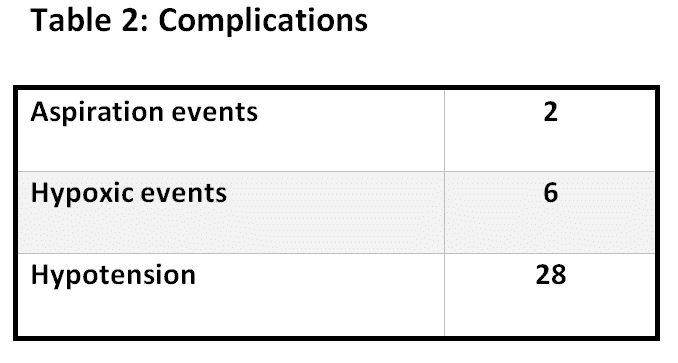
Results: Results are represented in table 1 and 2. Two regurgitations were noted, one with the use of succinylcholine, one with a high dose of rocuronium. Six hypoxic events (SaO2 below 90 during induction), and 28 hypotensive episodes were noted.
Discussion: Over time, incidence of RSII and use of succinylcholine decreased. Our limited data collection demonstrates no change in complication rate when cRSII is used versus RSII. This “controlled” technique is preferred at our institution. A prospective analysis is underway.

Powered by Eventact EMS