
Emergency Treatment of a Ruptured Giant Aneurysm in a Saphenous Vein Graft
An asymptomatic physically active 66-year old male with a history of coronary artery bypass
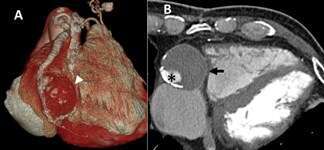
surgery and mitral valve replacement underwent cardiac CT angiography (CCTA) to evaluate the
patency of the bypass grafts. CCTA revealed a giant 4x4 cm aneurysm of an ectatic saphenous
vein graft (SVG) to the posterior descending artery (PDA) (Figure 1). Due to the patient’s lack of symptoms and the perceived risk associated with surgical or percutaneous treatment of the aneurysm it was decided to follow him non-invasively. One month later the patient sustained an inferior STEMI with a cardiac arrest. Emergency angiography revealed
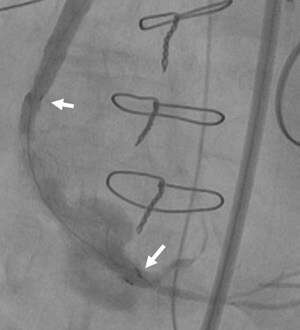
rupture of the SVG aneurysm (Figure 2) with occlusion of the PDA and echocardiographic
evidence of tamponade. Following stenting of the PDA, the coronary guidewire was
exchanged for an 0.035” guidewire via a Guideliner catheter. The 6F femoral sheath was exchanged for a 9F sheath (90 cm length) which was inserted into the SVG over the 0.035” guidewire. Following deployment of a 9x60 mm fluency stent graft within the SVG across the mouth of the ruptured aneurysm (Figure 3) the patient stabilized hemodynamically with ST-segment resolution on the EKG. The patient remained unconscious due to anoxic brain damage and died 1 month later. Early treatment of asymptomatic SVG aneurysms should be considered to avoid aneurysm rupture

Powered by Eventact EMS