
Was Two-Dimensional Strain for Diagnosing Chest Pain in the Emergency Room (2DSPER) a Negative Study Because of Poor Image Quality?
Background: Two-Dimensional Strain for Diagnosing Chest Pain in the Emergency Room (2DSPER) was a prospective multicenter study designed to determine whether 2D longitudinal strain (2DLS) can assist in triage of patients with chest pain in the emergency department (ED). In that study 2DLS was not useful to rule out acute coronary syndromes (ACS) in the ED.
Our aim in the present substudy was to determine the effect of 2D image quality on the diagnostic accuracy of 2DLS for ACS.
Methods: We reviewed apical views used for 2DLS analysis in all 605 patients included in the 2DSPER study. Studies with the best image quality, defined as optimal visualization of all left ventricular segments throughout the cardiac cycle, were categorized as HighQ (n=177), and compared with the lower quality group (LowQ, n=428). Abnormal 2DLS was defined as PSS20%>-17% (PSS20% being the peak left ventricular systolic strain value identifying the 20% worst strain values).
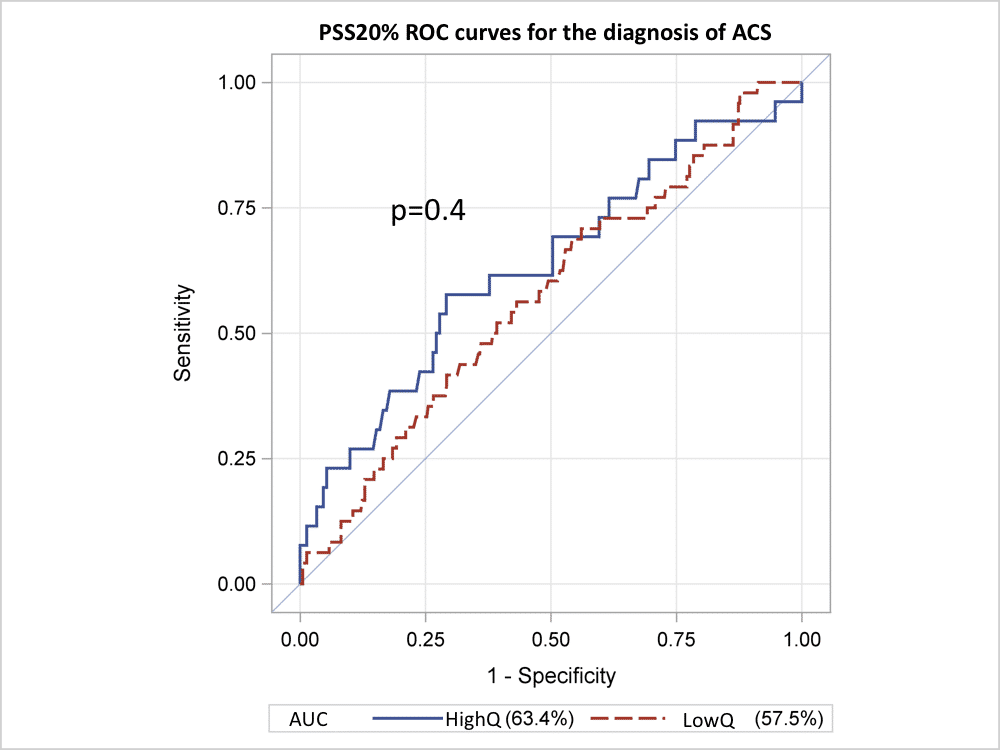
Results: ACS was diagnosed in 26/177 patients of the HighQ group (15%) and 48/428 (11%) of the LowQ group (p=0.3). The sensitivity of PSS20%>-17% for ACS was 73% for HighQ vs. 85% for LowQ (p=0.2), specificity 38% vs. 22% (p<0.0001), positive predictive value 17% vs. 12% (p=0.2), negative predictive value 89% vs. 92% (p=0.5) and overall accuracy 43% vs. 29% (p=0.0004). Although LowQ independently predicted abnormal 2DLS (OR 1.9, 95%CI 1.3-2.9, p=0.003), there was no significant difference between the receiver operating characteristic curves of PSS20% for ACS in the two groups (Figure) and abnormal 2DLS did not predict ACS in the HighQ group (OR 1.7, 95%CI 0.7-4.3, p=0.3).
Conclusions: Although the diagnostic accuracy of 2DLS for detecting ACS in the ED was significantly higher in patients with optimal image quality, it remained low and not clinically useful even in this subgroup of patients.

Powered by Eventact EMS