
Intraprocedural Valve-in-Valve Implantation for Treatment of Paravalvular Leak Following Transcatheter Aortic Valve Replacement: A Tailored Approach
Objectives: To assess the role of intraprocedural valve-in-valve (VIV) implantation for treatment of aortic regurgitation (AR) following transcatheter aortic valve replacement (TAVR) in relation to the site of deployment of the initial valve.
Background: AR following TAVR may be due to incorrect device positioning. VIV may decrease the grade of AR, however the specific mechanism of benefit has not been defined.
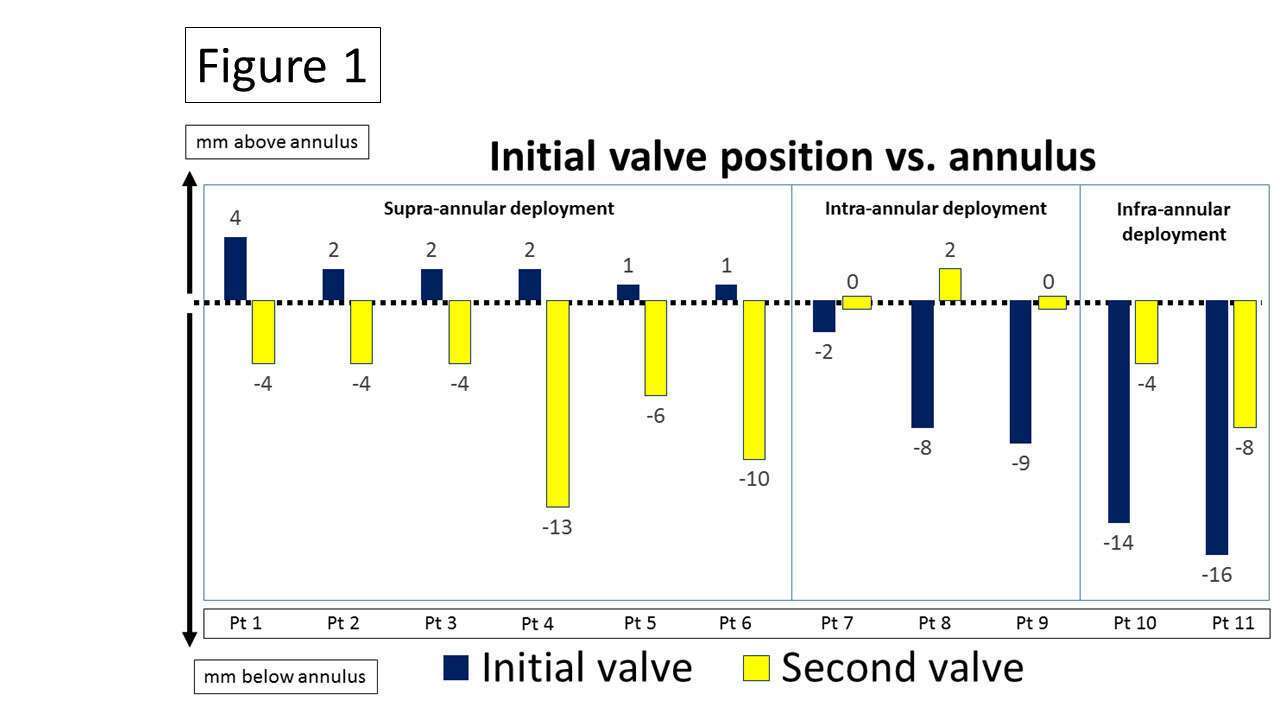
Methods: Patients with significant AR following implantation of self-expanding valves who underwent VIV were classified according to the position of the initial valves. Valve deployment was classified as supra-annular, intra-annular or infra-annular according to the location of the device pericardial skirt in relation to the aortic annulus. Positioning of second valves relative to the initial ones and their effect on the final AR grade were assessed.
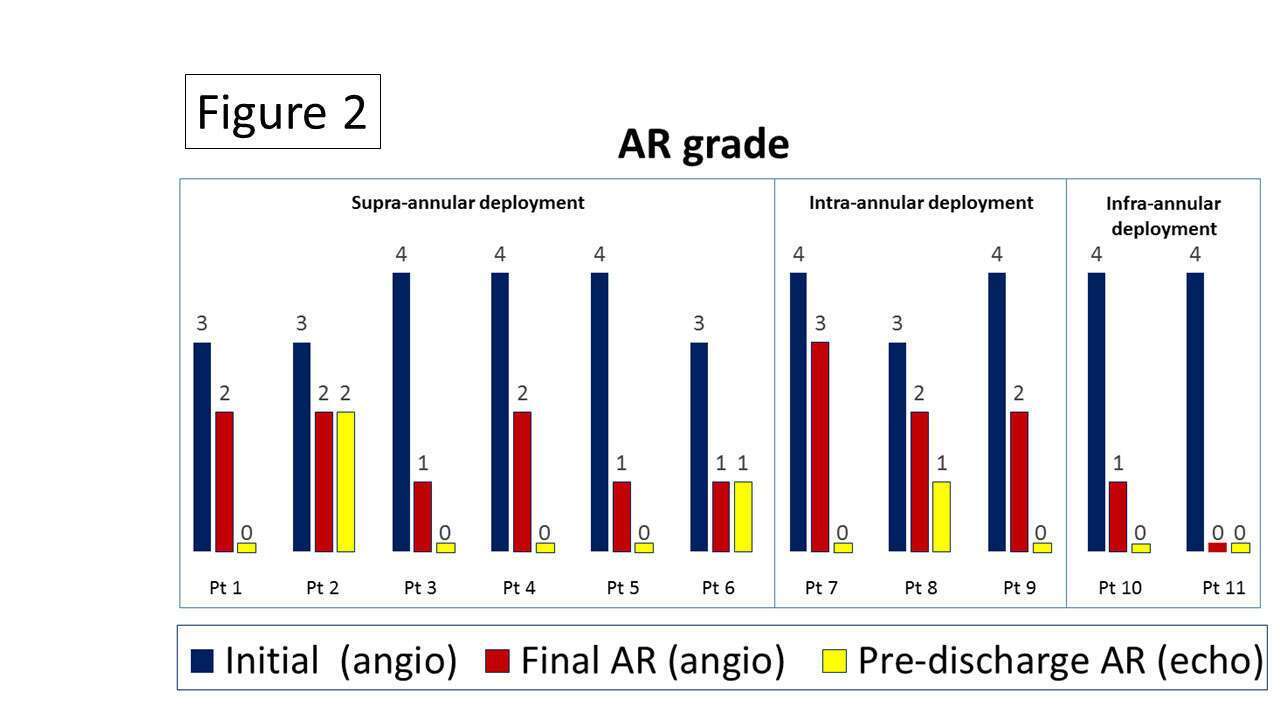
Results: Among 285 TAVR patients who received Corevalve or Evolut-R valves (Medtronic, USA), 11 (3.8%) underwent VIV due to AR. The initial valves were supra-annular in 6 cases (group-1), intra-annular in 3 cases (group-2) and infra-annular in 2 cases (group-3). In group-1 the second valves were implanted lower than the initial ones. In group-2 the second valves were implanted at the same level as the initial ones or higher. In group-3 the second valves were implanted higher than the initial ones (Figure 1). Following VIV the AR grade was reduced in all 3 groups (Figure 2).
Conclusions: VIV is a useful method for decreasing AR grade during TAVR procedures. Positioning of the second valve should be guided by the position of the initial valve relative to the annulus.
Powered by Eventact EMS