
Retrograde Femoral Artery Stent Graft Implantation for Treatment of Access Site Bleeding Following Transcatheter Aortic Valve Replacement
Objectives: To assess the feasibility of a retrograde approach for stent graft implantation for treatment of access site bleeding following transfemoral transcatheter aortic valve replacement (TAVR).
Background: Access site bleeding is a common complication of transfemoral TAVR. Percutaneous stent graft implantation may achieve hemostasis in these cases and avoid need for vascular surgery, however failure to advance a guidewire antegradely across the femoral artery may preclude stent delivery. We describe a cohort of patients in whom retrograde guidewire advancement following distal arterial puncture facilitated stent graft delivery.
Methods: A prospective TAVR registry was analyzed. Of 349 patients who underwent TAVR, 332 (95%) cases were performed via transfemoral access. Access site injury requiring stent graft implantation occurred in 56 (17%). In 4 (7%) patients antegrade wiring across the site of vascular injury was not possible and a retrograde approach for stent delivery was utilized.
Results: Distal vascular access was achieved via the superficial femoral or profunda arteries. Retrograde advancement of a polymer-coated 0.035” wire to the abdominal aorta, followed by stent graft delivery to the common femoral artery, was achieved in all cases. During a median (IQR) follow-up period of 198 (618) days (range: 46-2455) there were no deaths and no patients required additional vascular interventions.
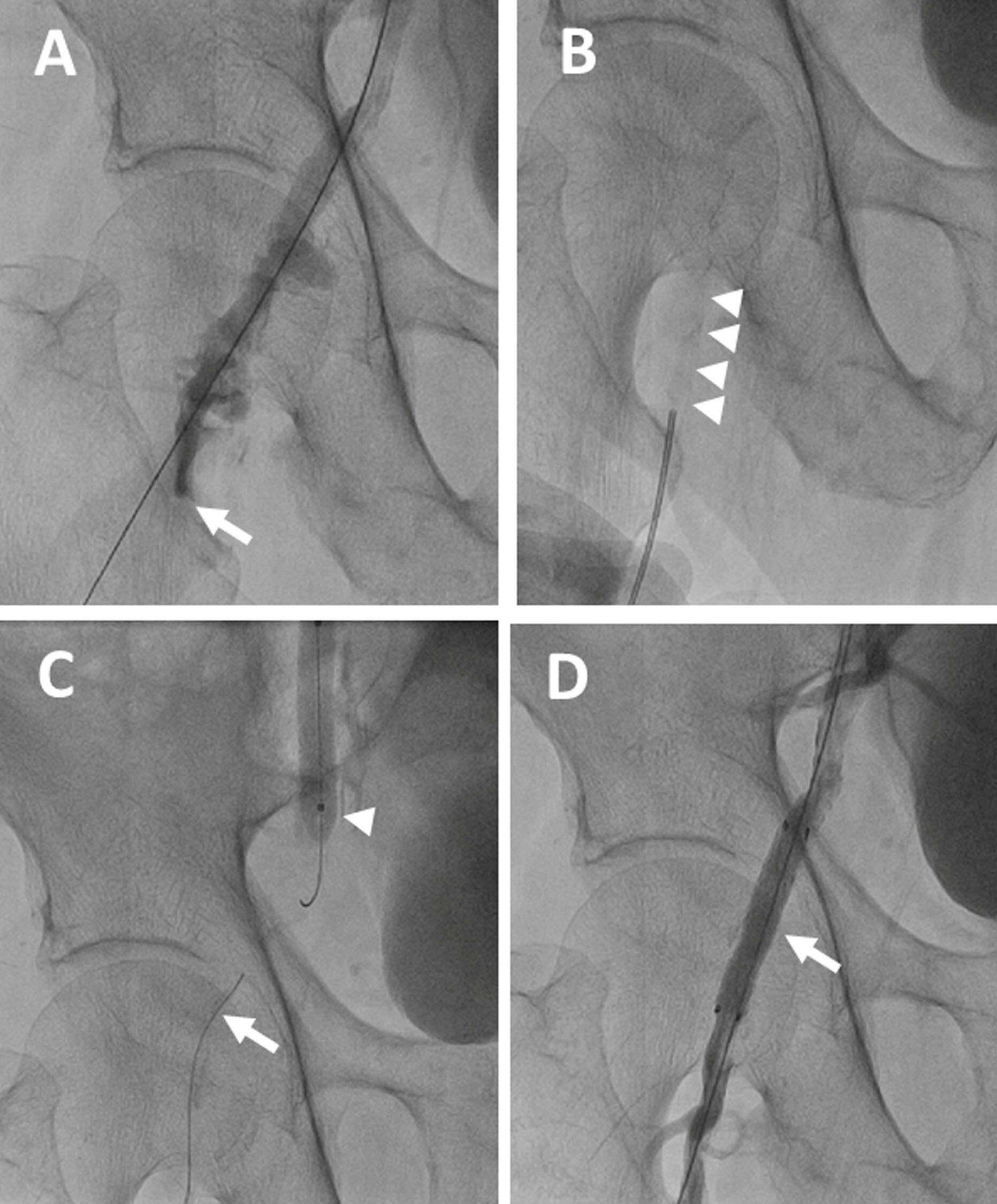
Representative case of retrograde stent graft delivery (Figure): A) Right femoral artery perforation (arrow). B) Insertion of a Seldinger needle into the calcified superficial femoral artery (SFA, arrowheads) under fluoroscopic guidance. C) Retrograde advancement of a 0.035” guidewire from the SFA (arrow) towards the occlusive balloon inflated in the common femoral artery (arrowhead). D) Final angiogram of the stented femoral artery (arrow).
Conclusions: A retrograde approach for stent graft delivery is feasible and allows percutaneous treatment of common femoral artery injuries following TAVR in patients who are not suitable for the conventional antegrade approach.
Powered by Eventact EMS