
Percutaneous Closure of a Giant Fistula with Two Aneurysms from Left Main Coronary Artery to Main Pulmonary Artery
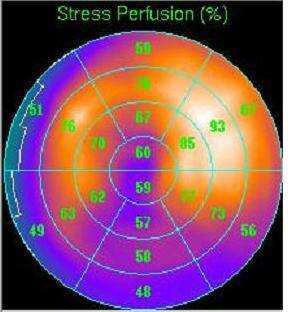
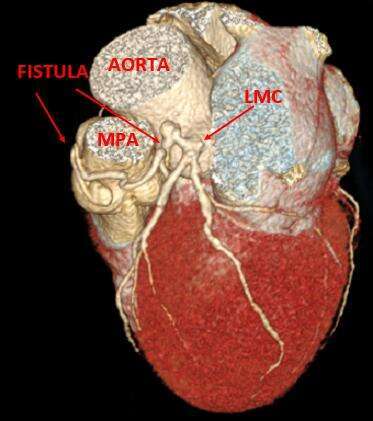
A 72-year-old man was admitted with recent onset angina and dyspnea on effort. Results of the physical examination were unremarkable. Electrocardiography revealed normal sinus rhythm with complete right bundle branch block. Trans-thoracic echocardiography revealed mild reduction of left ventricular systolic function and a calculated ejection fraction of 50%. Single-photon emission computed tomography (CT) thallium study confirmed the presence of a moderate reversible perfusion defect in the territory of the left anterior descending coronary artery (LAD) (Figure 1). Coronary arteriography revealed a large coronary artery fistula extending from the left main coronary artery (LMCA) to the main pulmonary artery (MPA). No obstructive coronary disease was found. Thus, the fistula was considered responsible for the symptoms and for the myocardial ischemia (Figure 2). Cardiac CT revealed a torturous fistula with two aneurysms – the distal one was connected to the MPA. The proximal aneurysm had a proximal short stump connected to the LMCA (Figure 3).
Therapeutic strategies were discussed with the patient and he preferred a percutaneous intervention and closure of the fistula. The fistula was selectively incubated using a Guiding Catheter and a guide wire was passed to protect LAD. Guide wire was introduced into the fistula and a micro catheter was passed over it successfully. Two coils with diameters greater than that of the fistula, and a vascular plug were deployed, leading to closure of the fistula with 0 TIMI flow (Figure 4).
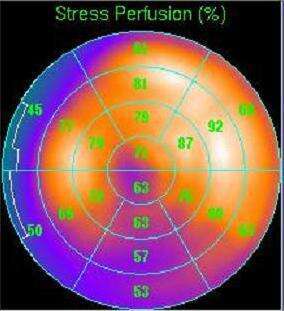
The procedure of closure of the giant fistula from the LMCA to MPA was successfully performed without any complications. The patient was discharged the following day. At the 3-month clinical follow-up, the patient was symptom free, and the SPECT thallium study revealed normal perfusion in the LAD territory (Figure 5).
Coronary arteriovenous fistula (CAVF) is a rare anomaly most commonly connecting between coronary artery to a cardiac chamber or adjacent vessel. CAVFs are present in 0.002% of the general population and are visualized in nearly 0.25% of patients undergoing catheterization. [1-5] Most frequently, 50% of fistulas originate from the right coronary artery, 40% from the left ascending coronary artery and left circumflex, and only few from the LMCA. The most common site of drainage is the right ventricle and pulmonary trunk (41% and 17%, respectively). [4-5]. The steal phenomenon that cause myocardial ischemia occurs suddenly because of underlying cardiac disease or stenosis in the coronary artery tree. Noninvasive methods, such as transthoracic echocardiography, cardiac CT, are used to assess the anatomy, nonetheless a SPECT thallium test is used to determine the defect perfusion because of the steal phenomenon.
In the presented patient, the origin from the LMCA, drainage into MPA, 2 aneurysms in the fistula, and large size of the fistula leading to coronary steal are unusual. Despite these complications, percutaneous closure was feasible and successful.



Powered by Eventact EMS