
Characteristics and Long-Term Outcomes of Patients with Reduced, Mid-Range, and Preserved Ejection Fraction Following Hospitalization for Acute Heart Failure in a Contemporary Real World Setting
Aims: Recent ESC heart failure (HF) guidelines introduced a new mid-ranged left ventricle ejection fraction (LVEF) category. The purpose of the present study was to describe the clinical characteristics and long-term outcomes of patients hospitalized with acute HF categorized by LVEF, in large contemporary prospective tertiary center cohort.
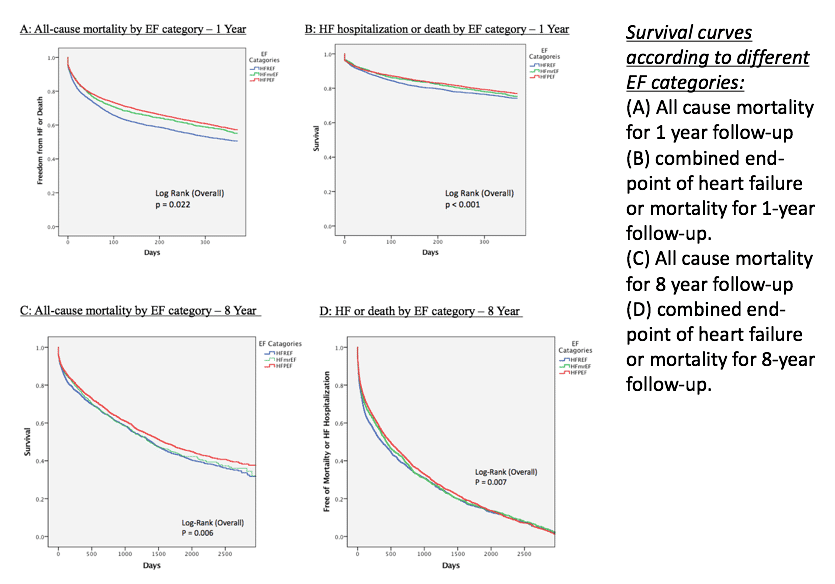
Methods and Results: A total 7,752 patients were included in this study. Patients were divided according to the recent ESC heart failure guidelines. Patients with preserved EF (HFpEF) compared to those with mid-range EF (HFmrEF) or reduced EF (HFrEF) were older, more likely to be female, had a higher frequency of comorbidities, including hypertension, diabetes mellitus, and anemia. Kaplan-Meier survival analysis (Figure) showed increased mortality rates at 1-and 8-years of follow-up in both the HFmrEF (24% and 48%, respectively) and HFrEF (25% and 47%, respectively) groups, as compared with the HFpEF group (22% and 41%, respectively; log-rank p-value =0.007 for the overall difference during follow-up). Consistently, multivariate analysis showed patients with HFmrEF experienced a significant higher risk for all-cause mortality (HR= 1.24, p=0.04) and HF or death (HR= 1.2, p=0.02) compared to the HFpEF group, and a similar risk to the HFrEF group. Systemic pulmonary artery pressure (SPAP) was an independent predictor for long-term mortality among all LVEF subgroups (HR 1.43, p<0.001).
Conclusion: Our findings suggest that acute HF patients with HFmrEF group have increased risk for long–term mortality and repeated HF hospitalization that is similar to those with HFrEF. Elevated SPAP is a powerful predictor for adverse long-term outcomes following hospitalization for acute HF.

Powered by Eventact EMS