
Femoral Versus Axillary Cannulation in Acute Type - A Dissection Repair Surgery
Objective: We compared early and late outcomes between patients who underwent femoral versus axillary cannulation for repair of acute type A aortic dissection.
Methods: Between 2004 and 2017, we retrospectively reviewed clinical outcomes of 135 consecutive patients who underwent emergency surgery for acute type A aortic dissection repair via femoral (n=84) or right axillary (n=51) artery cannulation. Mean patient age was 6312 years and 66% were male.
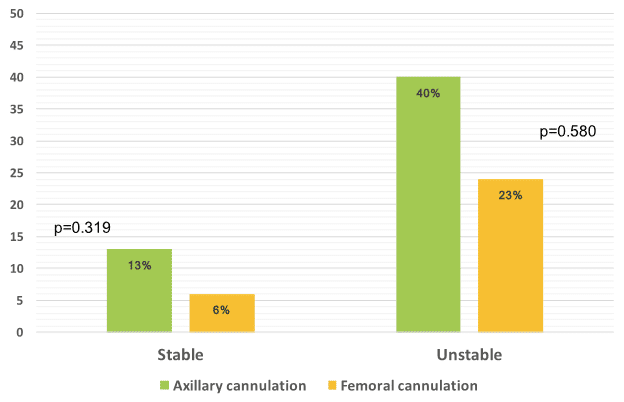
Results: Overall in-hospital mortality was 12.6% (axillary 15.7%, femoral 10.7%; p=0.430). Patients who underwent axillary compared to femoral artery cannulation had a non-statistically significant higher in-hospital mortality rate among stable and unstable patients (13% vs. 6.5%, p=0.319 and 40% vs. 22.7%, p=0.580; respectively) (Figure).While there was no difference in the major complication rates such as stroke, low cardiac output, and surgical revision, there was a higher incidence of renal failure that required dialysis in patients who underwent axillary cannulation (12% vs. 1%, p=0.012). Among those discharged from hospital, the 1, 2 and 3-year survival rate was 91%, 90% and 88% respectively.
Conclusions: Based on our experience, emergency surgery for both stable and unstable patients with acute type A aortic dissection demonstrated better survival and less renal impairment when using the femoral cannulation approach.

Powered by Eventact EMS