
Acute Kidney Injury Based on the KDIGO Among ST Elevation Myocardial Infarction Patients Treated by Primary Percutaneous Intervention
Objective: Acute kidney injury (AKI) is associated with adverse outcomes after acute ST elevation myocardial infarction (STEMI). The recently proposed KDIGO criteria suggested modifications to the consensus classification system for AKI, namely lower threshold of absolute serum creatinine increase and extending the time frame for AKI detection for up to 7 days. We evaluated the incidence, risk factors, as well as the long term mortality associated with AKI as classified by KDIGO definition in a large single center cohort of consecutive STEMI patients.
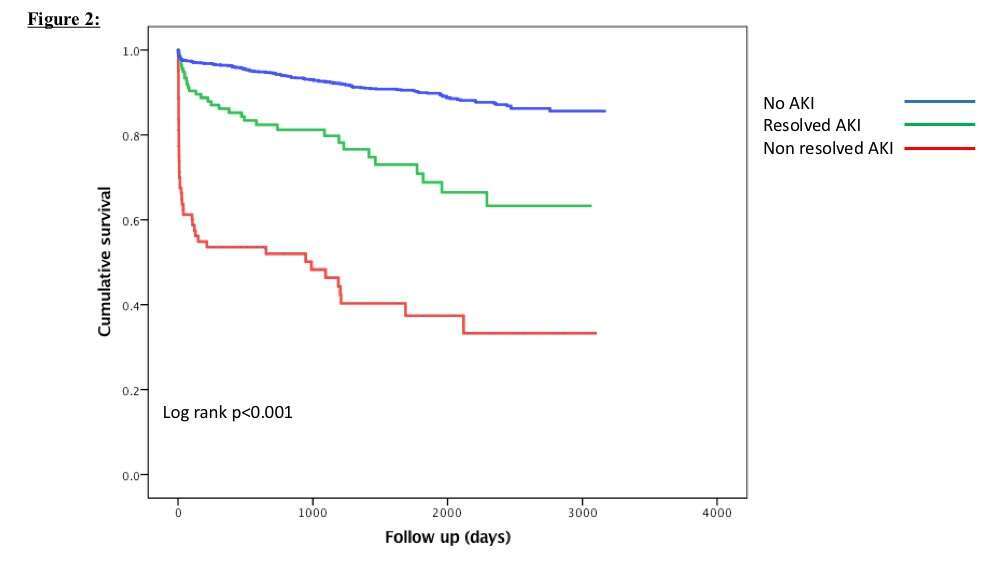
Study design and methods: We retrospectively studied 2122 consecutive STEMI patients undergoing primary percutaneous coronary intervention (PCI). Recruited patients were admitted between January 2008 and May 2016 to the Cardiac intensive care unit with the diagnosis of acute STEMI. We compared the utilization of KDIGO and consensus criteria for the diagnosis of AKI, and its relation to long term mortality.
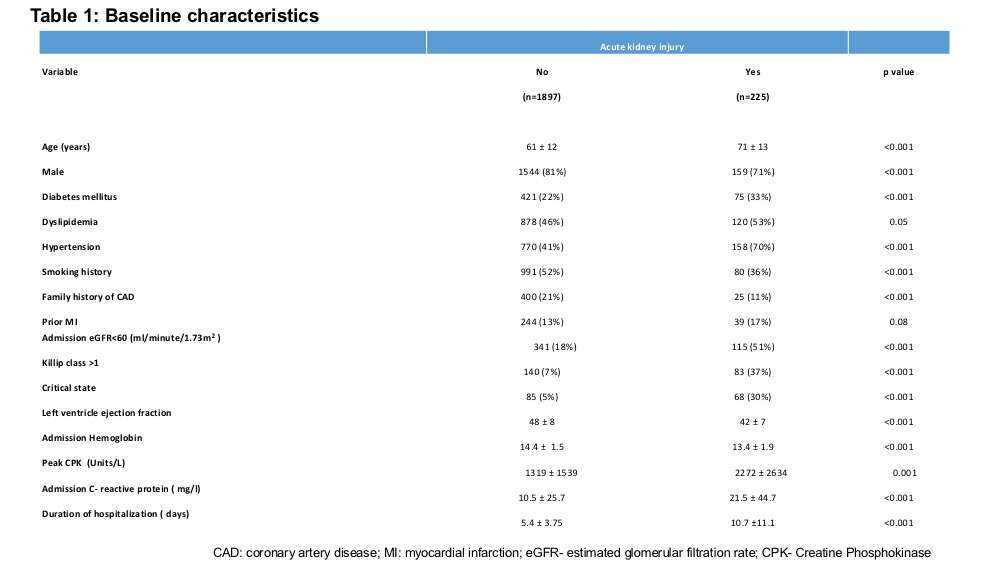
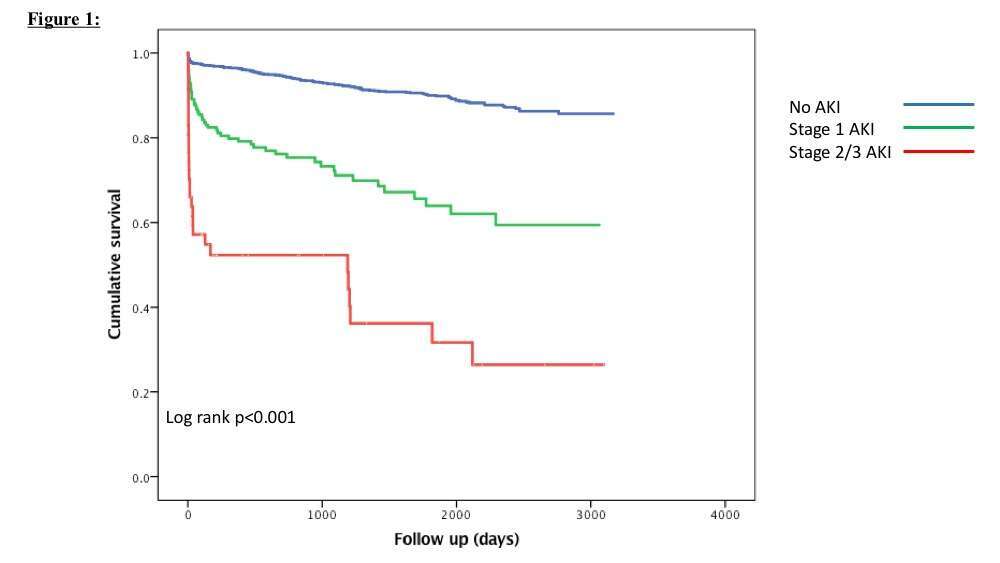
Results: The KDIGO criteria allowed the identification of more patients as having AKI (10.6% vs. 5.6%, p<0.001) compared with the consensus criteria. Even mild elevation of serum creatinine (> 0.3 mg/dl) was associated with marked increase in all-cause mortality (HR 4.7, 95% CI: 3.1-6.43, p<0.001). Patients with AKI having resolution of their renal function prior to hospital discharge had still significantly higher mortality compared to patients with no AKI (23% vs. 8%, HR 3.1,95% CI: 2.09-4.90, p<0.001).
Conclusions: KDIGO criteria is more sensitive in defining AKI compared with the consensus criteria in STEMI, and identifies at risk population for adverse long term outcomes.
| Click the link to view image: | https://events.eventact.com/dan/29113/104182.jpg |

Powered by Eventact EMS