
Echocardiographic E to E Prime Ratio: An Incremental Predictor of Clinical Outcome in Cardiovascular Patients Irrespective of Left Ventricle Ejection Fraction
Background: The ratio between early mitral inflow velocity and mitral annular early diastolic velocity (E/e`) on echocardiography is the best non-invasive estimation of LV (left ventricle) filling pressures. E/e` provides prognostic information in cardiovascular diseases. We evaluated its prognostic significance in relation to LV systolic function.
Methods: All hospitalized cardiovascular patients with an echocardiography examination during 5 years were evaluated. Patients with significant (moderate or worse) valve disease were excluded.
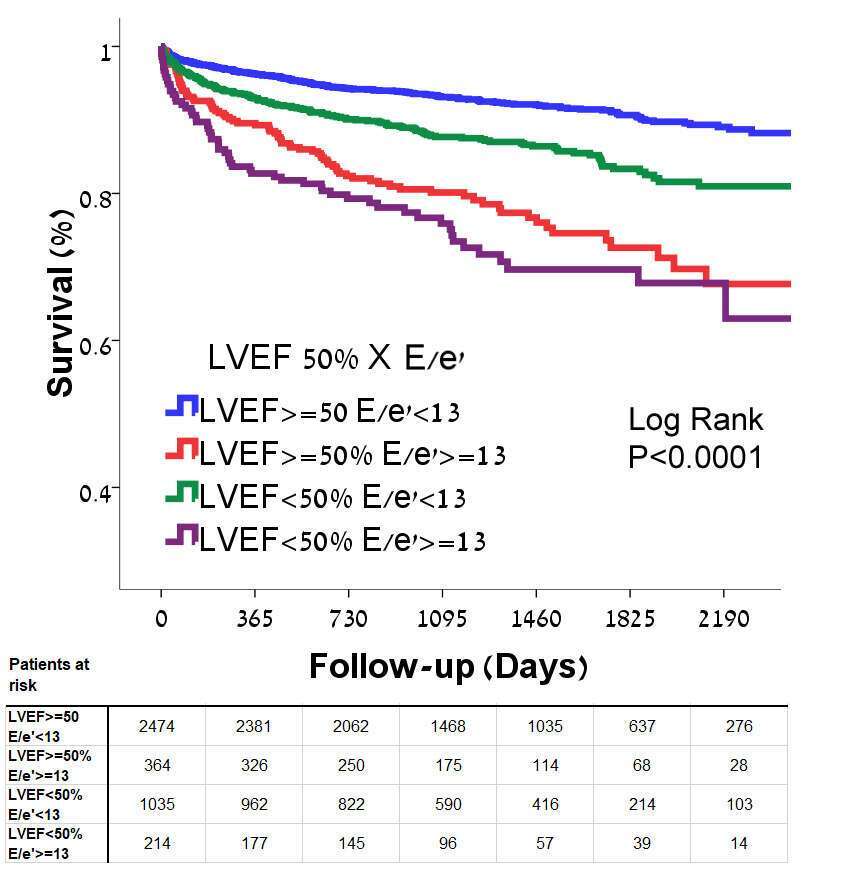
Results: A total of 4087 patients met inclusion criteria. Median age was 63 (IQR 53-73), 2835 (69%) males. 1249 patients (31%) had reduced LVEF (EF<50%) and 578 (14%) had elevated LV pressures (E/e`≥13). Median follow-up was 1,365 Days. Overall mortality was 11.8%. Patients with elevated LV pressures had a significant shorter median survival compared to patients with equivocal/normal LV filling pressures (i.e. E/e`<13) (74.5±2.0% vs. 90.7±0.5%, Log Rank P<0.001). Cox regression analysis after adjustment for age and gender, demonstrated that patients with E/e`≥13 had a 2 fold increase in mortality rates (HR 2.05, 95% CI 1.69-2.49, P<0.001). The prognostic significance of E/e`>13 was incremental and more pronounced than LVEF: Classification according to LVEF and LV pressures demonstrated that survival was lowest in patients with elevated LV pressures regardless of LVEF. Patients with EF≥50% and E/e`≥13 had a lower survival rate compared to patients with EF<50% and E/e`<13 (77.4±2.4% vs. 87.0±1.1%, P<0.001; Figure). Adjustment for age and gender demonstrated the same finding: E/e`≥13 in patients with EF≥50% was an independent predictor of mortality compared to E/e`<13 with EF≥50% (HR 2.05, 95% CI 1.57-2.67, P<0.001) and higher than patients with reduced LVEF and E/e`<13 (HR 1.71, 95% CI 1.38-2.13, P<0.001).
Conclusions: Elevated LV pressure as evaluated by echocardiography is an important prognostic tool in hospitalized cardiovascular patients. It is a significant incremental predictor of increased mortality regardless of LV ejection fraction.
| Click the link to view image: | https://events.eventact.com/dan/29113/104212.jpg |

Powered by Eventact EMS