
Penetrating Cardiac Stab Wound: Case Report and Diagnostic Algorithm
Penetrating cardiac trauma (PCT) represent a major surgical challenge because of mortality rate ranging from 40 to 90 %. In PCT the right ventricle (RV) is more frequently involved.
Case Report. At work, a 57-year-old man attempted suicide self-inflicting scissors stab wound in the chest (Fig. 1) . He was found unconscious, in a pool of blood. On the ambulance, a FAST showed an important left pleural effusion, his vital parameters were blood pressure (BP) 100 mmHg and cardiac pulse 110/min. At his arrival in Emergency Department, BD was 80-90 mmHg, volume reintegrated and an Angio Computed Tomography showed pericardial effusion and left hemithorax (Fig. 2). Left anterolateral thoracotomy in fifth intercostal space, blood was removed and the left lung deflated in order to open the pericardium: blood pressure fell < 50 mmHg. The pericardium was incised, a big clot was removed, three epicardial injuries were on anterior RV. One of them was actively bleeding 1 cm beside the left anterior coronary artery; this lesion was sutured using 4.0 polypropylene reinforced with Teflon strip (Fig. 3). Afterward, three parenchymal lesions were sutured on the anterior aspect of the superior left lung lobe using polypropylene 4.0. The patient recovered uneventfully, on sixth postoperative day he was transferred to a psychiatric unit. At 6-month follow-up he is doing well returning to work.
Discussion. We illustrate an algorithm (Fig. 4) in emergency cases considering all variables found in these patients and identifying risk factors for death. The “cardiac box” is the area where all PCT may determine an injury to the heart structures and to the great vessels (Fig. 5). Consider always the diaphragm as a moving target: an injury that on first glance may look abdominal is actually intrathoracic. In our case, FAST evaluation allowed a prompt diagnosis and emergency lifesaving surgery.

Fig. 1. . Self-inflicted scissors stab wound in a 57-year-old man who attempted suicide: thee scissors stab wounds are visible medially the left nipple.
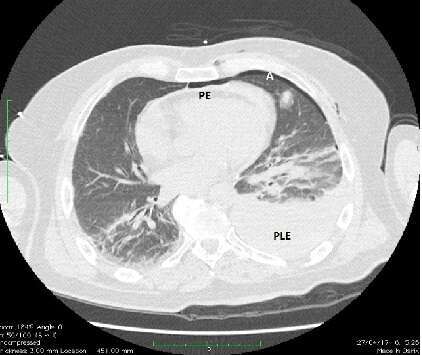
Fig. 2. Chest CT scan showing pericardial effusion (PE), a huge left pleural effusion (PLE) and air (A) in anterior mediastinum and anteriorly in the right pleural cavity.
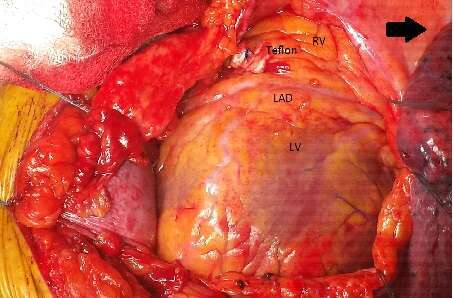
FIg. 3. Left anterolateral thoracothomy, in fourth intercostal space, suture of one right ventricle lesion with polipropilene 4.0 reinforced by Teflon strip., RV = right ventricle , LAD = left anterior descending coronary artery , LV = left ventricle; the black arrow indicates patient’s head.
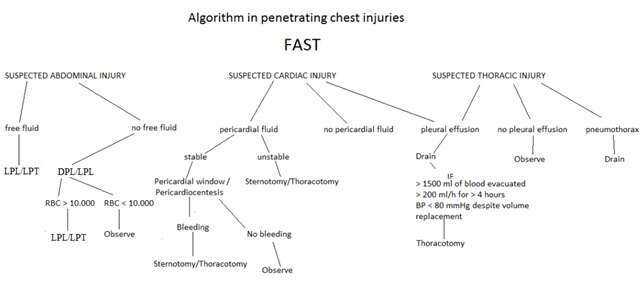
Fig. 4. Algorithm utilizing FAST for penetrating trauma to the torso. DPL=Diagnostic Peritoneal Lavage, LPL=Laparoscopy.
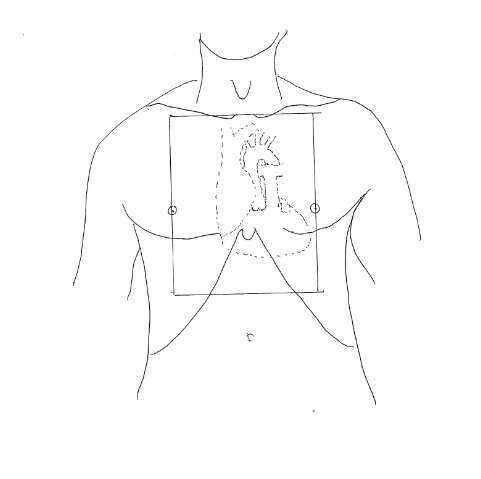
Fig. 5. The “cardiac box”: the area is delimited superiorly by the sternal notch, laterally by the nipples and inferiorly by a transverse line halfway between the xiphoid process and the umbilicus.

Powered by Eventact EMS