
PERMANENT PACEMAKER IMPLANTATION VIA THE LEFT SUPERIOR VENA CAVA TO A COLLATERAL
OF THE CORONARY SINUS LEADING TO THE LEFT VENTRICLE
Introduction. Sinus node disfunction, atrio-ventricular block and brady-tachy syndrome are frequent complications after Fontan correction. Patients
with prior extracardiac conduit are classically considered ineligible for transvenous atrial pacemaker implantation due to lack of venous access to the
atrial myocardium with the need of an epicardial implantation. However, the epicardial approach requires general anesthesia and a thoracotomy.
Case report. A 21 old male patient, who underwent at 3 years of age extracardiac Fontan with PFTE patch operation for morphologically left univentricular heart with persistent left superior vena-cava (LSVC), was admitted to our Center for atrial tachycardia with signs of congestive heart failure. An electric cardioversion after flecainide treatment resulted in a sinus pause, followed by slow junctional rhythm. In the next week the patient alternated junctional rhythm to symptomatic atrial tachycardia. So we decided to implant a PM to achieve a pharmacological arrhythmias control safety. To avoid a surgical implantation, which was considered at high risk for the clinical condition of the patient, we decide to implant an endocardial lead through the persistent LSVC in a collateral of the coronary sinus (CS).
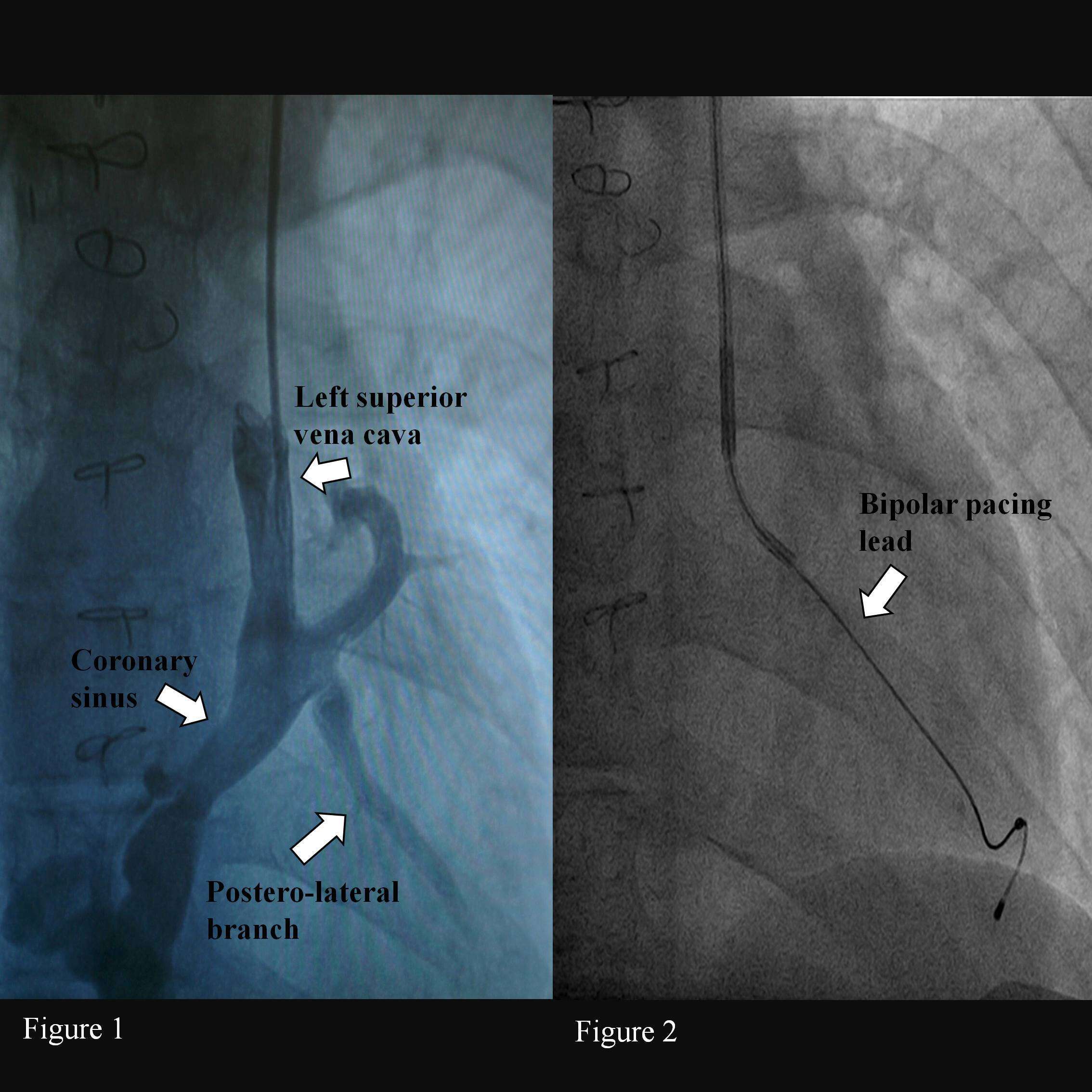
Pacemaker implantation. After left axillary vein puncture a guide was inserted in the LSVC. Through a peel-away 9 Fr introducer an angiography was performed. The angiography showed the presence of a wide CS with a postero-lateral collateral straight on (fig.1). A CRT sub-selection catheter was introduce in the ostium of the
CS collateral. A CRT Bipolar lead was positioned in a distal branch of the vein (Medtronic ATTAIN ABILITY™ 4296 ) (fig. 2). No complication occurred. After 3 months the lead showed normal electrical values and low threshold (1 V/0,4 ms).
Conclusion. Endocardial PM implantation through persistent LSVC to a collateral of the CS revealed to be an effective and safe approach for Fontan patients. Connections between the venous system and the coronary sinus may turn out to be very useful and should be surgically preserved when possible for later electrophysiological interventions.
Powered by Eventact EMS