
Pre-Ablative Scoring System for Prediction of Recurrence after PVI with Cryo-Balloon and Optimization of Ablation Strategy
Background: Several scoring systems for prediction of post ablation recurrence were recently presented. Aim of this study was development of new scoring system for prediction of long term recurrences after PVI with cryo-balloon new generation (CBA) based only on non-invasively assessed data.
Methods: A total of 952 patients ablated with CBA in our institution since May 2012 and completed follow up >3 month were enrolled in the study. n 110 patients additionally to PVI roof line (RL) was performed at discretion of physician. The endpoint of this study was the first documented recurrence of atrial tachyarrhythmia (>30 sec.). The patients receiving PVI (n=843) only were randomized to two cohorts: 1) training set (n=421) and 2) validating set (422) Finally, score was calculated in PVI+RL group
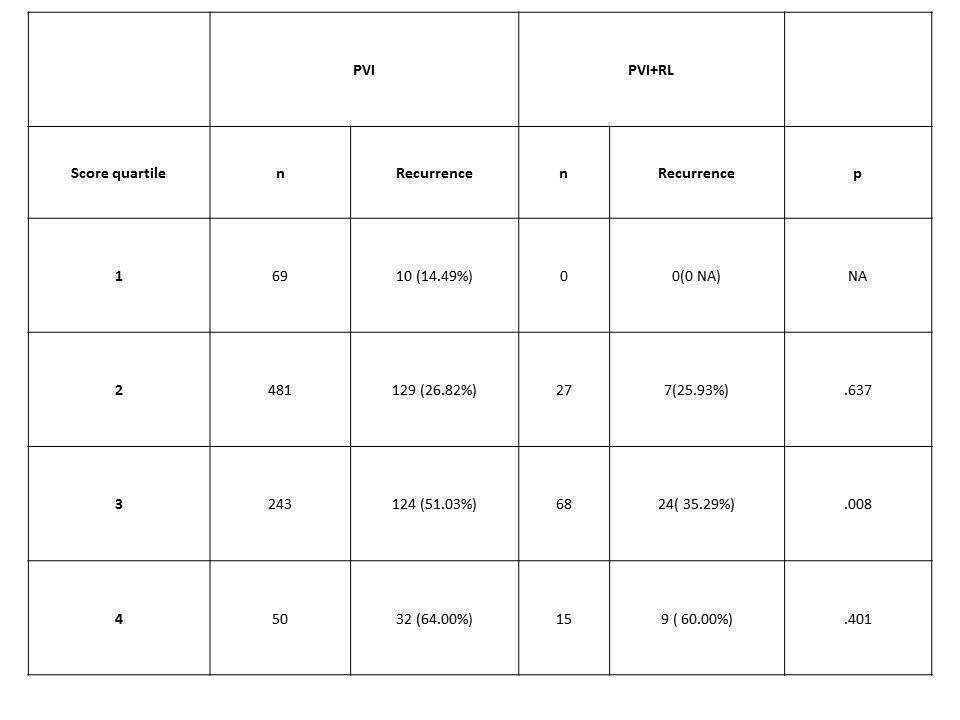
Results: Out of 843 patients with PVI only 295 (35%) reached endpoint within follow up of 28 (12-45) months. In training set (128 endpoints) follows variables were revealed to be predictive for recurrence: Female gender (b=0.328, HR=1.44 (1.21-2.044), non-paroxysmal AF (b=.659, HR=1.94 (1.37-2.74), TAPSE< 20 mm (b=0.563; HR= 2.20 (1.49-3.23)), History of MI (b=0.640 HR=(2.33 (1.49-4.31)), History of AF ((b=0,003; HR=1.002 (1.001-1.004))/month), LA area indexed by BSA (b=0.084; HR=1.086 (1.014-1.162)/cm2/m2). The median value of calculated score was 2.00 (1.67-2.44). The C-statistics of score in training set was .670 (.612-.728).. In the validating set the C-statistics of RSCPR was 680 (637-740), p=.638. In whole cohort C-statistics of score was .674 (636-730). The distribution of patients is shown the table.
Conclusion: Majority of enrolled patients had relative low risk of recurrence and performing of RL did not improve outcome in these patients, in contrast in patients with score ≥3 quartile additional RL improved outcome with higher significance. Prospective randomized study with including criteria based on score ≥3 should be initiated for evaluation of impact of the cryo-RL.
Powered by Eventact EMS