
PAC-induced Ventricular Fibrillation
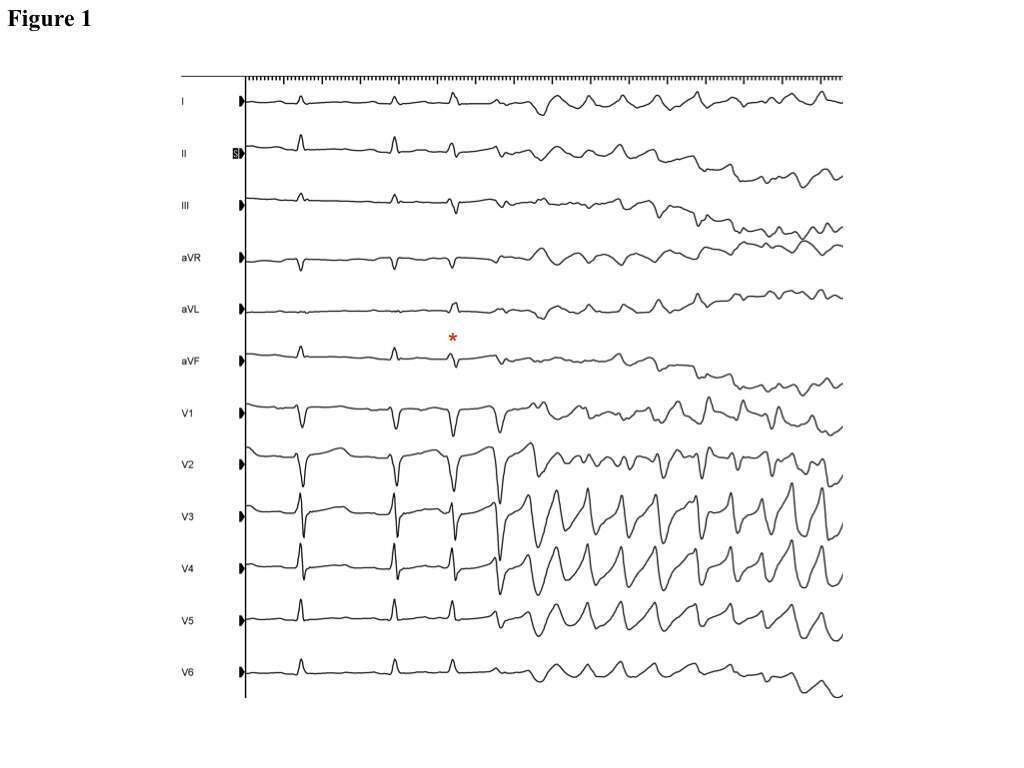
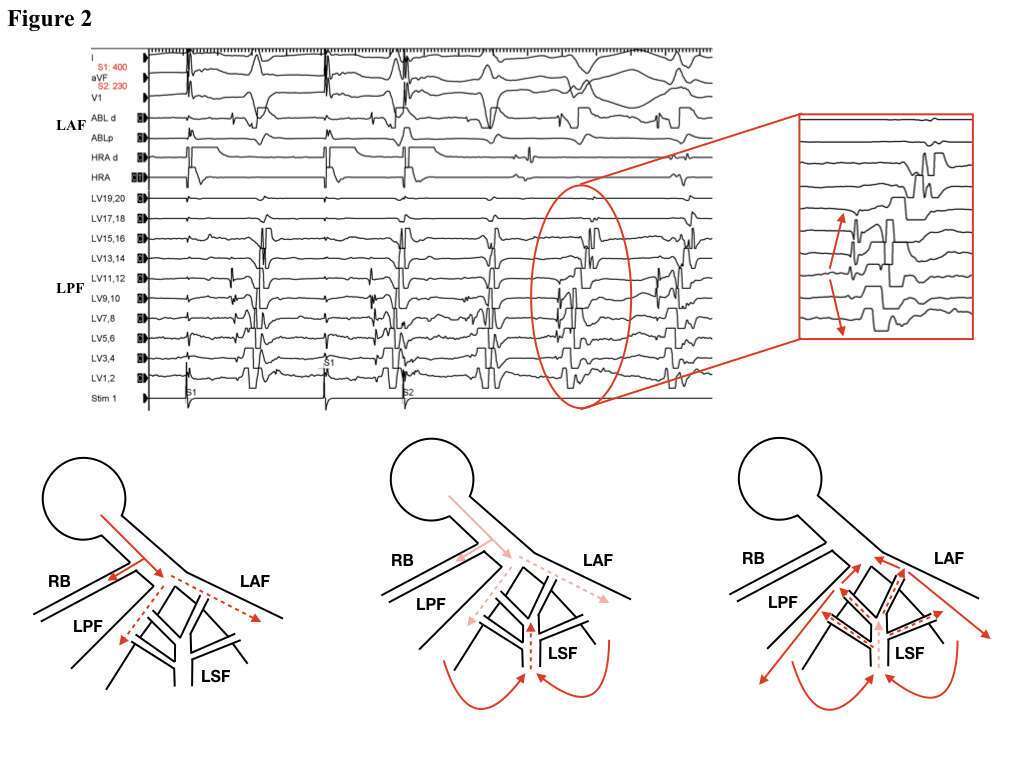
A 29-year-old man with no past medical history presented after an aborted cardiac arrest. He was noted to have an episode of left posterior fascicular (LPF) VT and underwent cardiac evaluation which was unremarkable. He was referred for EP study at which point spontaneous episodes of VF were observed (Figure 1). All episodes were initiated by a PAC, which resulted in QRS aberrancy (Figure 1 asterisk) followed by VT/VF. This sequence was easily reproducible with atrial extrastimulation. QRS aberrancy and the pattern of His-activation were suggestive of left-sided fascicular involvement. A duodecapolar catheter was positioned on the LPF and then on the LAF, and the stereotypic pleiomorphic ventricular beats were observed with atrial extrastimulation. The second ventricular beat after the A2 stimulus followed eccentric activation of the LPF (Figure 2, top panel) and of the LAF. This suggested utilization of a middle septal fascicle with near-simultaneous and eccentric activation of the anterior and posterior fascicles. We then proceeded with linear ablation across the LPF and into the mid-septum, targeting the middle septal fascicle. Following this, there were no episodes of spontaneous or atrial extrastimuli-induced VT/VF. A repeat EP study was performed a few days later without any further VT/VF.
The induction of fascicular tachycardia from the atrium has been well described, however the finding of PAC-induced VF is unique. We hypothesize that the premature atrial beat resulted in relative delay within the complex arborization of the left septal fascicle (Figure 2, bottom panel). This led to eccentric but near-simultaneous activation of both anterior and posterior fascicles resulting in re-entry with subsequent destabilization of multiple micro-reentrant fascicular circuits resulting in VF. The utilization of the left-sided conduction system was confirmed when VT/VF could not be induced after extensive ablation of the posterior and septal fascicles.
Powered by Eventact EMS