We report a cerebellitis case with severe ataxia and encephalopathy likely precipitated by an acute viral illness in a 3-year-old girl with a past medical history of seizures managed with topiramate until one month before her current admission.
On admission the patient was febrile to 38.40C and appeared ill. The neurological exam was significant for Pediatric GCS 11. Lab tests showed elevated CRP (118.1 MGR/L). Otherwise normal tests including Blood cultures and toxicology screen.
Computed tomography of the head was normal. She had CSF mild pleocytosis and a culture without growth.
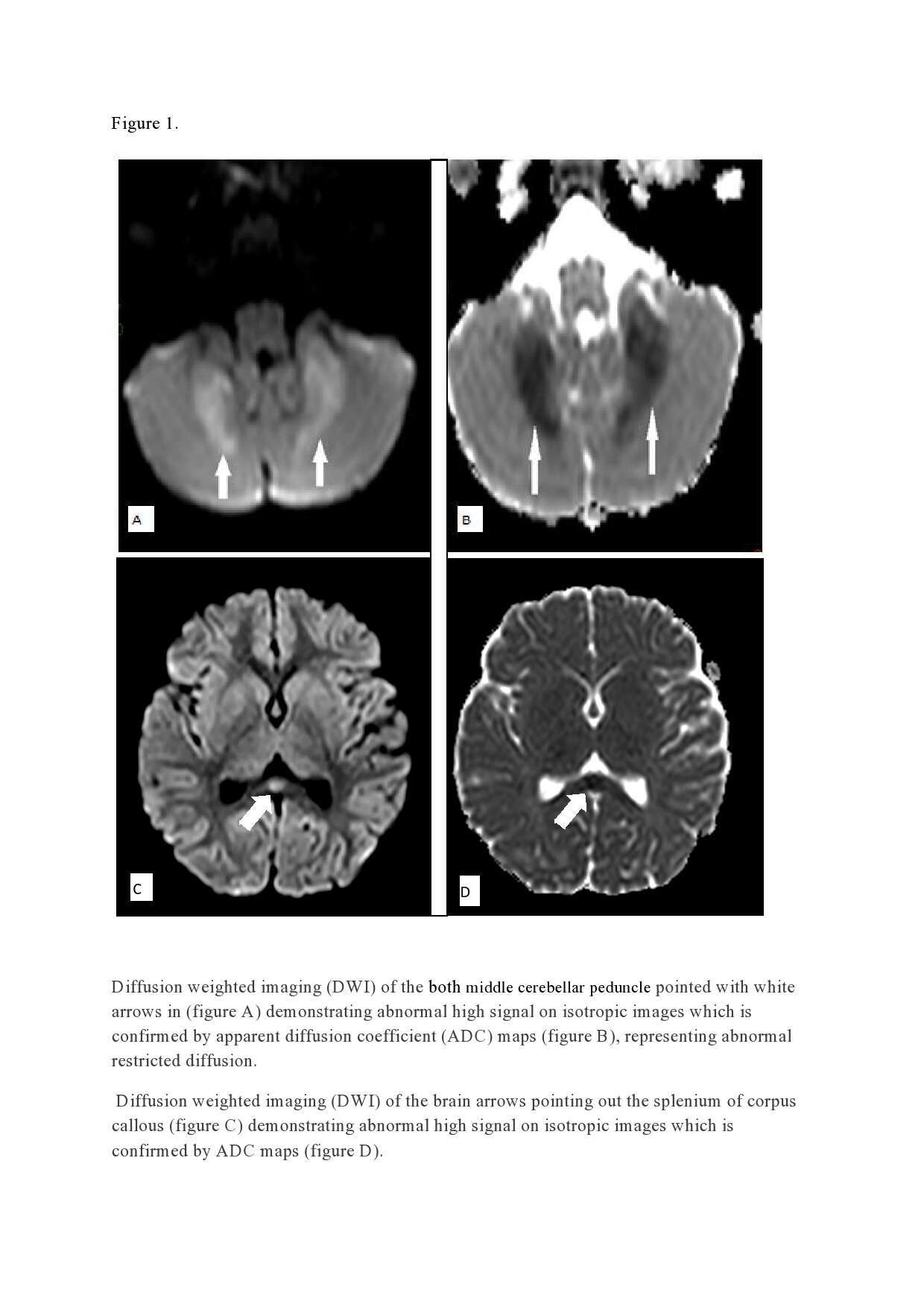
Her electroencephalogram showed no apparent epileptic activity. Brain and spinal cord magnetic resonance imaging and Diffusion weighted imaging demonstrated restricted diffusion of cerebellum and the corpus callosum splenium .
She was treated with high dose parenteral corticosteroids and then Intravenous Immunoglobulin with improvement in her neurological status. Additionally, since urinary excretion of 3-hydroxyisovaleryl carnitine was elevated, biotin supplement was administered. Notably, at one-month follow-up, her neurological exam was normal and she had returned to her baseline activities.
This case raises questions about biotin deficiency and CNS vulnerability, with a unique pattern of CNS involvement seen in MRI. More specifically, it suggests the need for further research aimed at investigating whether such patients may be more prone to CNS infection, and in particular cerebellitis. It also suggests the need to better understand the mechanisms underlying the impact of biotin deficiency on the human immune system and how and when such a deficiency may increase the risk of infectious disease.