Both symptomatic and asymptomatic newborns with congenital CMV (cCMV) are at risk of developing sensorineural hearing loss. Still, universal screening for cCMV is not routine with most institutions pursuing CMV testing only with specific indications.
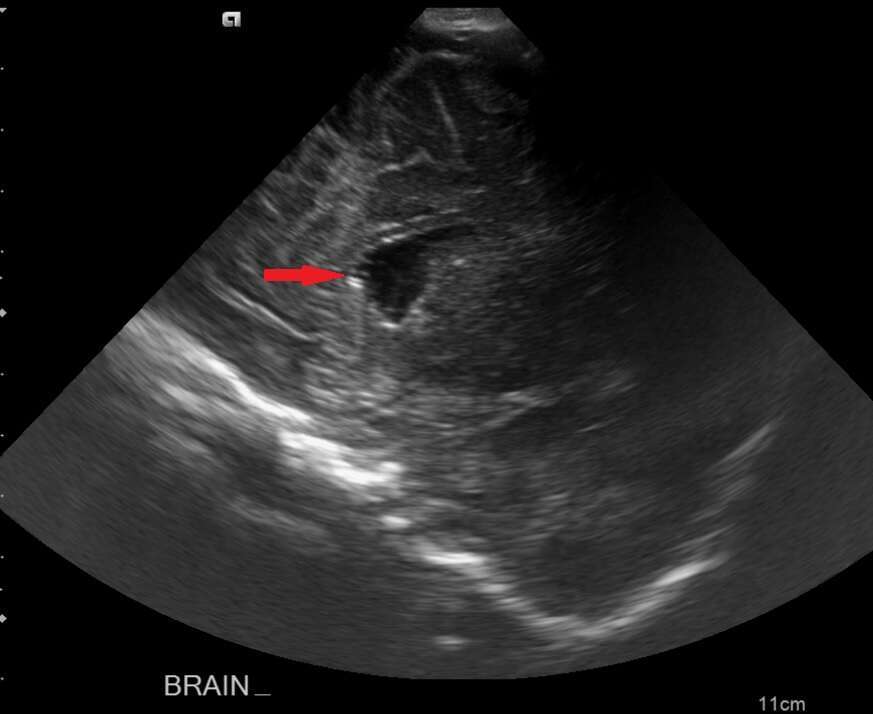
We describe a 2.5-month-old full-term male infant, admitted with a 2-day history of high fever and decreased intake. The infant appeared ill; accordingly, a full sepsis work-up was performed and significant for an abnormal CBC [WBC, 30K (ANC 18K), HgB 10, Platelets 522 K], CRP 77 and bloody cerebrospinal fluid (CSF) which partially cleared. The patient was started on meningeal doses of ampicillin and ceftriaxone. Blood, urine and CSF cultures were all without growth. Given the patient`s persistent fever and ill appearance, further lab investigation was performed on the CSF yielding PCR CMV detection (BioFire). Notably, at birth, the head circumference was on the third percentile; OAE screen normal. This concerning constellation prompted a complete evaluation for cCMV. Brain ultrasound showed periventricular calcification in the anterior horn of the lateral ventricles without hemorrhage, a significant finding suggestive of severe symptomatic cCMV disease. The ophthalmologic and neurological examinations were unremarkable. The infant’s urine was +PCR CMV; Guthrie card negative; maternal serology CMV IgG positive, IgM Negative. His brain evoked auditory response was normal. After considerable deliberations, the patient was started on valgancyclovir and advised multidisciplinary follow-up.
This case highlights under-recognition of cCMV thereby delaying institution of antiviral therapy. Moreover, it is instructive in demonstrating CMV as an infectious etiology in the febrile young ill infant.
