Background: Diagnosing bacterial pneumonia is challenging. Currently, many clinicians obtain chest radiograph imaging (CXR) to establish diagnosis and need for antibiotic therapy. However, this tool does not reliably distinguish bacterial from viral etiologies and is subject to variable interpretation. Here, we evaluate the potential of an immune-signature (Srugo et al. 2017) to reduce CXR in children suspected for pneumonia.
Methods: We studied children enrolled in ‘Pathfinder’, a double-blinded multinational study designed to validate an immune-signature that distinguishes viral and bacterial infections based on TRAIL/IP-10/CRP proteins (index-test). Infection etiology was assigned by unanimous expert panel following review of patients’ clinical, laboratory, radiological and microbiological data. CXRs were classified according to radiologist interpretation, labeled according to WHO methodology.
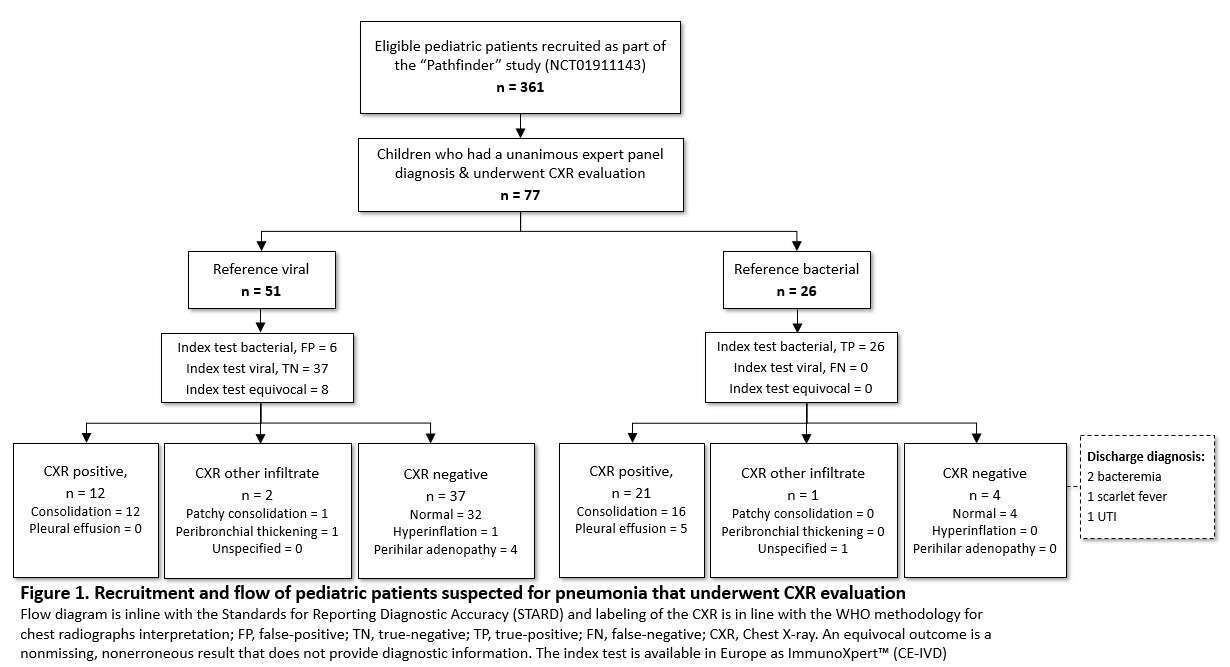
Results: 244 of 361 children were assigned reference etiology; 77 underwent CXR evaluation for suspected pneumonia (Figure 1). Positive/other CXR findings were observed in 36/77 children - 14 reference-viral, 22 reference-bacterial. Negative CXR findings were observed in 41/77 children - 37 reference-viral, 4 reference-bacterial. The index-test’s PPV for bacterial infection was 81.3% (95% CI: 67.4%-90.1) and the NPV 100%; i.e., no child exhibiting a viral index-test result was reference-bacterial. These findings suggest that, based on a viral index-test result, almost half of CXRs could be avoided (from 77/244=31.6% to 40/244=16.4%, P<0.001).
Conclusion: Positive and negative radiographic findings do not necessarily reflect underlying infectious etiology. With high NPV and PPV, the TRAIL/IP-10/CRP signature has potential to reduce CXR rates in children suspected for pneumonia. Implementation studies are required to evaluate utility in safely decreasing CXR.