
Comparison of Outcomes of Degenerative Mitral Valve Repair Surgery for Anterior, Posterior and Bileaflet Pathology
2Cardiology, Sheba Medical Center
Background: Degenerative mitral valve (MV) disease with anterior leaflet (AL) pathology is considered less favorable compared to isolated posterior leaflet (PL) pathology, with reference to durability. Our objective was to compare outcomes of patients who underwent MV repair for bileaflet (BL), PL and AL pathology, and to investigate predictors for repair failure.
Methods: Between 2004 and 2018, 592patients underwent MV repair with or without concomitant tricuspid valve repair due to degenerative disease: 361 (61%) had PL pathology, 192 patients (32%) had BL pathology and 39 (7%) had AL pathology. Mean age was 56±12, 53±14 and 56±18 years in PL, BL and AL pathology groups, respectively (p= 0.016). Clinical and echocardiographic follow-up was complete.
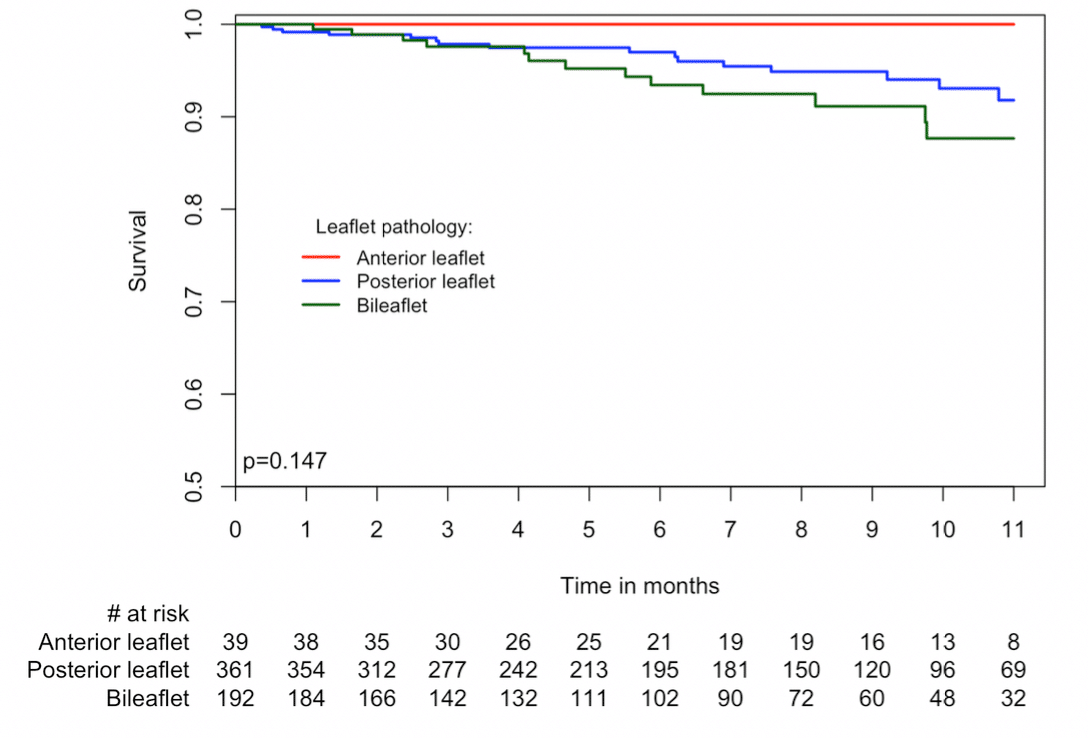
Results: There were no cases of in-hospital deaths in the entire cohort. The mean clinical follow-up was 61±46 months (1 to 167) and echocardiography follow-up was 46±42 months (1 to 163). Freedom from reoperation was 93% (336/361), 92% (176/192) and 87% (34/39), and there were 16 (4.4%), 13 (16.8%) and 0 (0%) late deaths (Figure), in the PL, BL and AL groups (NS). Late echocardiography revealed that 75%, 83% and 77% of patients (PL, BL and AL groups, respectively) were free from moderate or severe mitral regurgitation (MR) (p=0.157). Predictors for recurrent significant MR or reoperation were: more symptomatic patients with greater preoperative NYHA functional class (grade III-IV vs. I-II) (OR 1.86 95% CI 1.19-2.88, p=0.006), and when the repair did not include annuloplasty (OR 0.24 95% CI 0.06-0.82, p=0.022) or included resection of the posterior leaflet (OR 1.72 95% CI 1.12-2.65, p=0.014).
Conclusions: MV repair can be achieved with excellent early results. Long-term outcomes and reoperation rates for AL and BL pathologies are not significantly different from PL pathology.

Powered by Eventact EMS