
Long-term Risk Stratification of Patients Undergoing Coronary Angiography According to the TIMI Risk Score for Secondary Prevention (TRS-2P)
2Community Medicine and Epidemiology, Lady Davis Carmel Medical Center
3Faculty of medicine, Technion, Israel Institute of Technology
Background: A risk score for secondary prevention after myocardial infarction (TRS-2P) was recently developed from the TRA2°P-TIMI 50 trial based on 9 established clinical factors (age≥75, hypertension, diabetes, smoking, kidney dysfunction, peripheral artery disease, heart failure, prior stroke and prior CABG), classifying the risk for major adverse cardiovascular events (MACE). We aimed to evaluate the performance of TRS-2P for predicting long-term outcomes in real-world patients presenting for coronary angiography.
Methods: Retrospective analysis of 13,593 patients that were referred to angiography for the assessment or treatment of coronary artery disease between 2000 and mid-2015 in a single center. Risk stratification for 10-year MACE (myocardial infarction, ischemic stroke or all-cause death) was performed using the TRS-2P score, divided into 6 categories (0 to ≥5 points), and in relation to the presenting coronary syndrome.
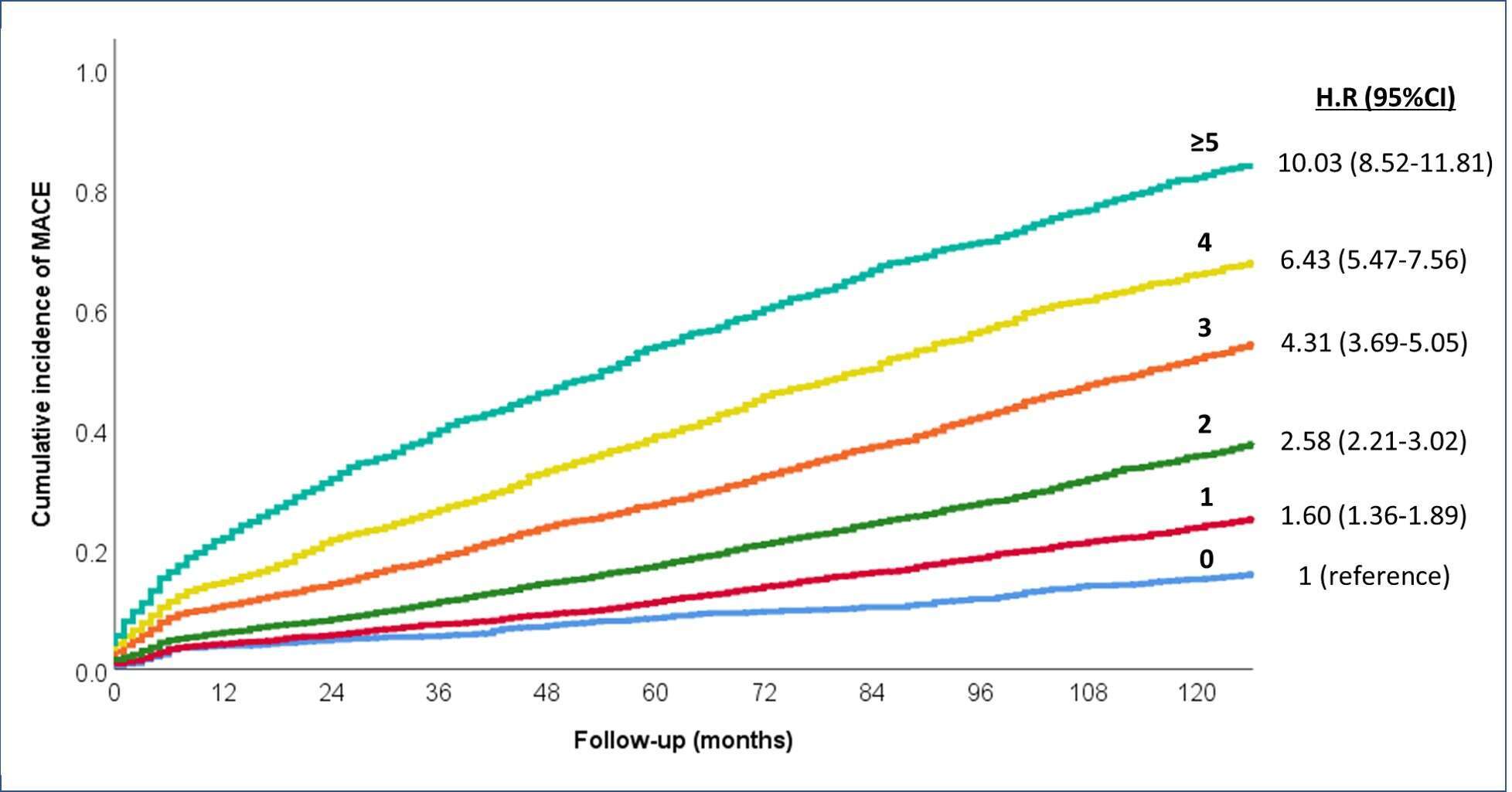
Results: All clinical variables, except of prior CABG, were independent risk indicators. The annualized incidence rate of MACE increased in a graded manner with increasing TRS-2P score, ranging from 1.65 to 16.6 per 100 person-years (ptrend<0.001). The pattern was similar for 10-year cumulative incidence of MACE (Figure). Compared to the lowest-risk group (risk indicators=0), the hazard-ratios (95% CI) for MACE were 1.60 (1.36-1.89), 2.58 (2.21-3.02), 4.31 (3.69-5.05), 6.43 (5.47-7.56) and 10.03 (8.52-11.81), in those with 1,2,3,4 and ≥5 risk indicators, respectively. Risk gradation was consistent across the individual clinical endpoints. The risk score showed fair discrimination with c-statistics of 0.704 for MACE and 0.735 for mortality. The graded relationship between the risk score and event rates was observed in both patients presenting with acute and non-acute coronary syndromes.
Conclusions: The use of TRS-2P, a simple risk score based on routinely collected risk indicators, enables risk stratification in patients undergoing coronary angiography. Its predictive value is demonstrated in real-world setting with long-term follow-up, and regardless of the acuity of presentation.
Powered by Eventact EMS