
Temporal Trends in Oral Anticoagulation Therapy in Non-valvular Atrial Fibrillation
2Clalit Research Institute, Clalit Research Institute, Chief Physician's Office, Clalit Health Services
Aims: Oral anticoagulation therapy (OAC) reduces the risk of embolic stroke and is associated with reduced risk of mortality in patients with non-valvular AF (NVAF) but is underused in clinical practice. The purpose of this study is to evaluate the change in purchasing patterns of OACs (both warfarin and NOACs) over time in NVAF patients according to stroke and bleeding risk.
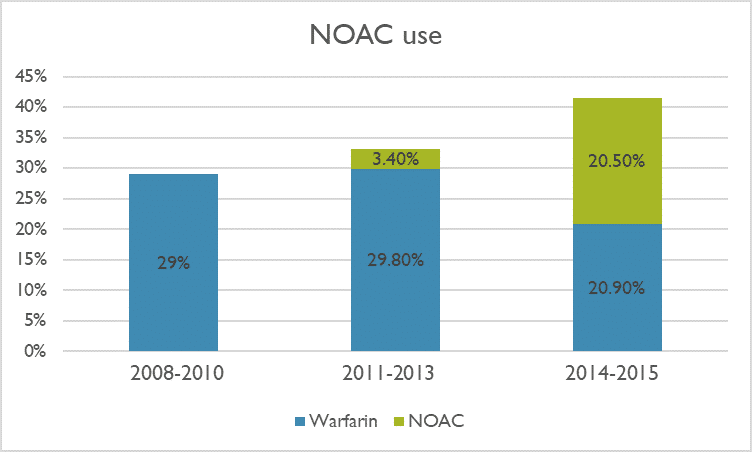
Methods and Results: We conducted a prospective, historical cohort study using the Clalit Health Services electronic medical records database. The study population included all Clalit members ≥ 25 years old, with a new diagnosis of NVAF between 2008 and 2015. A total of 58,385 cases were identified. The median age was 75 years and 52.3% were women. Most patients (86.4%) had a CHA2DS2-VASc score of 2 or more and 58.9% of patients had a HAS-BLED score ≥3. Between 2008-2010, 29% of patients purchased a vitamin K antagonist, the only available OAC at the time. OAC purchasing increased to 41.4% between 2014 and 2015 with half of patients purchasing a NOAC (Figure 1). The preference for NOAC was evident across the embolic risk spectrum: NOAC purchasing increased from 1.9% to 15% in those with a CHA2DS2-VASc of 0 and from 4.5% to 29.7% in those with a risk score of 1, while it increased from 10.9% to 51.8% among those with CHA2DS2-VASc≥ 2. Interestingly, patients at high risk for both stroke and bleeding, OAC purchasing also increased significantly from 35.7% in 2008 to 51.1% in 2015.
Conclusions: In this real-world population-based cohort of patients with newly diagnosed NVAF, we found a lower than expected rate of OAC prescription. Nonetheless, we detected an encouraging increase in OAC purchasing. Use of NOACs has risen exponentially in only a few years, accounting for a greater pool of AF patients being prescribed an OAC.

Powered by Eventact EMS