
Hypoxic Ischaemic Encephalopathy (HIE): An Audit of Assessment, Management and follow up In a Level 2 Neonatal Unit
Background: HIE is a significant cause of neonatal morbidity and mortality affecting 1.5 per 1000 live births. For moderate to severe HIE, evidence supports therapeutic hypothermia in improving survival and neurological outcomes.
Objective: Assessment of diagnosis and management of babies with HIE, and their neurodevelopmental outcome at 1 and 2 years.
Methods: Retrospective analysis of infants born at a level 2 unit in 2014 - 2016 with a diagnosis of HIE on the Badger system. Duplicates and babies
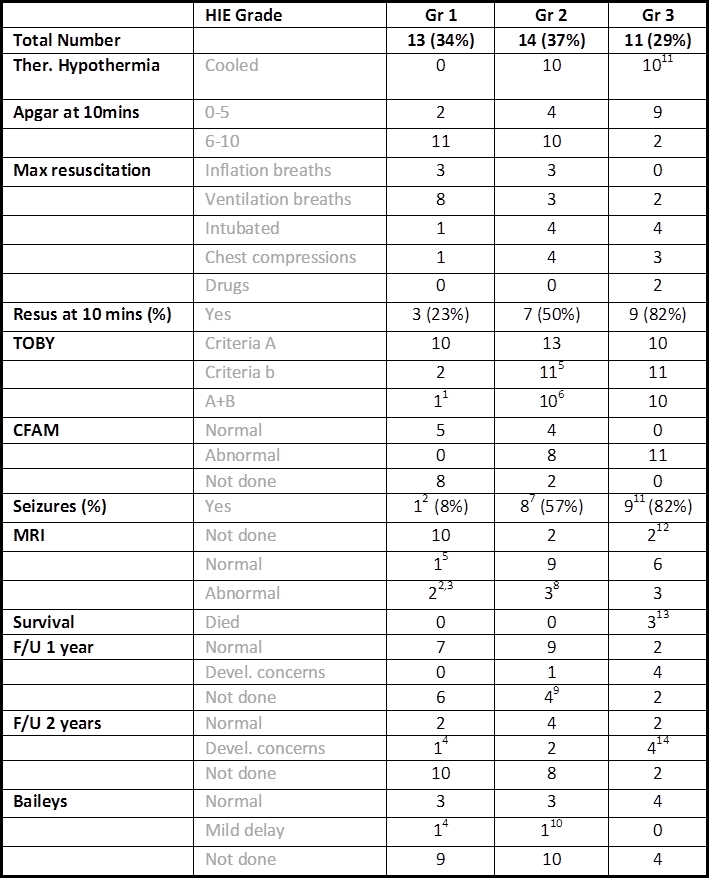
Results: 38 (0.3% of live births) were identified as HIE: grade 1- 34%; grade 2 - 37%; grade 3 -29%. 53% were cooled. 47% had seizures. 3 infants with grade 3 died.
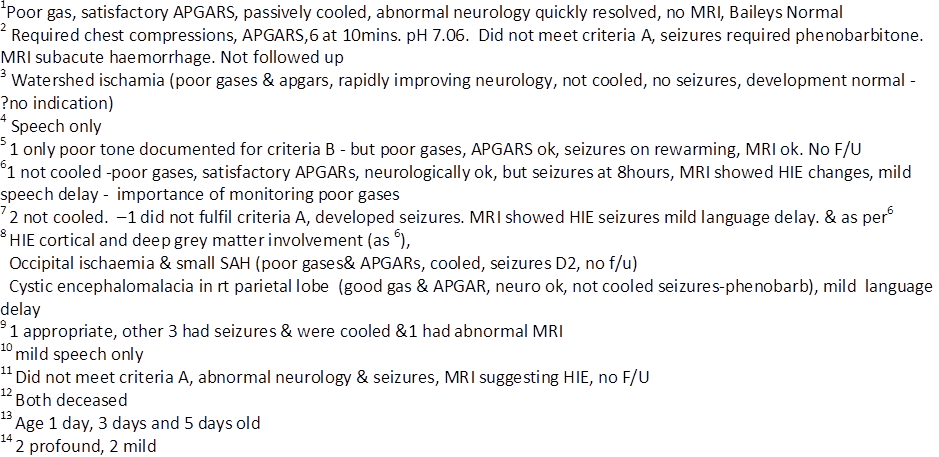
For grade 2 babies, 90% of the 10 cases where babies were cooled had normal MRI’s. 50% of the 4 babies not cooled had MRI changes and developmental delay.
The most common developmental concern in Grade 2 HIE was speech delay (15%).
1 patient with grade 2 had poor cord gases, but AGPARS 75, 910 and was initially neurologically intact so was not cooled, but developed seizures at 8 hours. MRI changes and mild developmental delay was observed at 2 years.
26% of HIE patients followed, including 1 with grade 1 HIE, had developmental delay.
18% of all grade 3 babies had profound delay, but 36% had a normal Baileys assessment at 2 years following cooling.
Conclusion: Developmental follow up is very important in HIE, particularly grades 2 and 3.
Grades 1 and 2 have good outcomes for survival and neurodevelopment.
Cooling should be carefully considered in grade 2 babies. Neurology should be observed closely in patients with poor gases, ensuring the window of opportunity is not missed.
Grade 3 babies can do well with cooling.
Powered by Eventact EMS