
Complete Surgical Resection and Total Rehabilitation of A Patient with High Flow Maxillary Arteriovenous Malformation
2Plastic Surgery, Albert Einstein Hospital
3Head and Neck Surgery, UNIFESP/ EPM
Objectives: To report a challenging arteriovenous malformation (AVM) located in the left maxilla region of a young patient, with severe oronasal bleeding, requiring radical resection and immediate reconstruction.
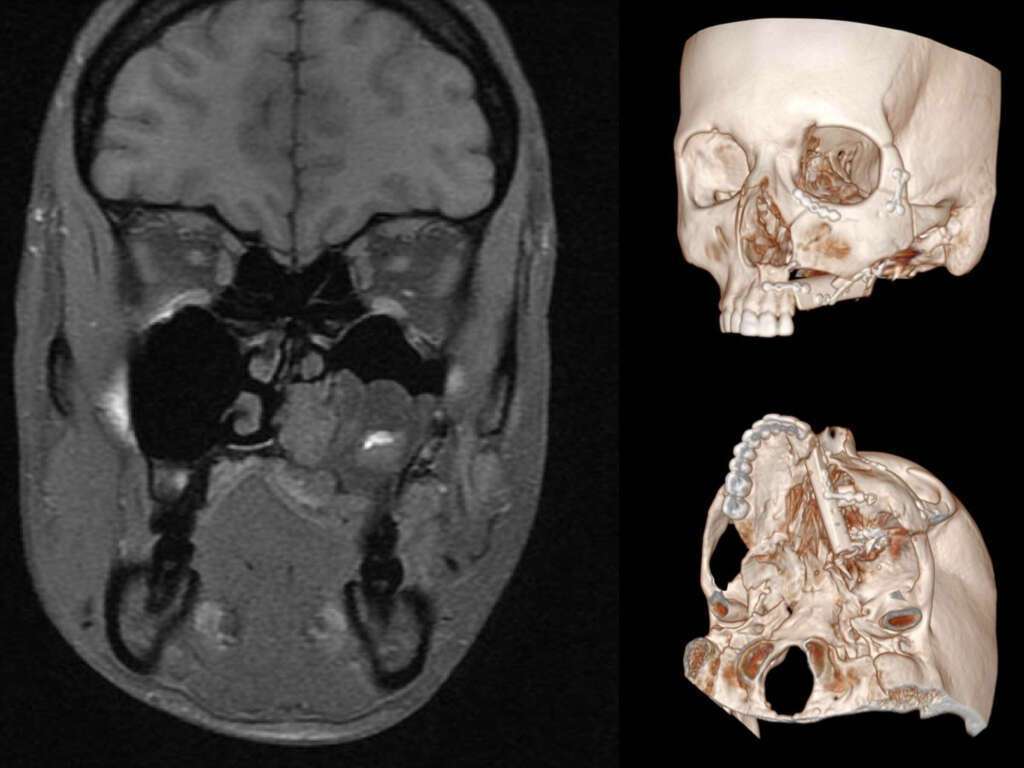
Methods: A previously asymptomatic 25 y.o. female reported her first hemorrhagic episode originated from left upper molar region, with hypovolemic shock, only controlled after embolization. Deformity of the palate, dental mobility and daily epistaxis demanded a second embolization. The deformity worsened after embolization. Arteriography, CT and MRI suggested an AVM, confirmed by biopsy.
A multidisciplinary team defined management by radical resection and immediate reconstruction. A modified facial translocation was performed to allow safe control of the nidus and feeding vessels, preserving the orbital floor and upper portion of the maxilla.
Complete AVM removal included resection of the alveolar bone lateral to the left upper incisors, hard palate, portions of the soft palate, pterygoid region and the left inferior turbinate.
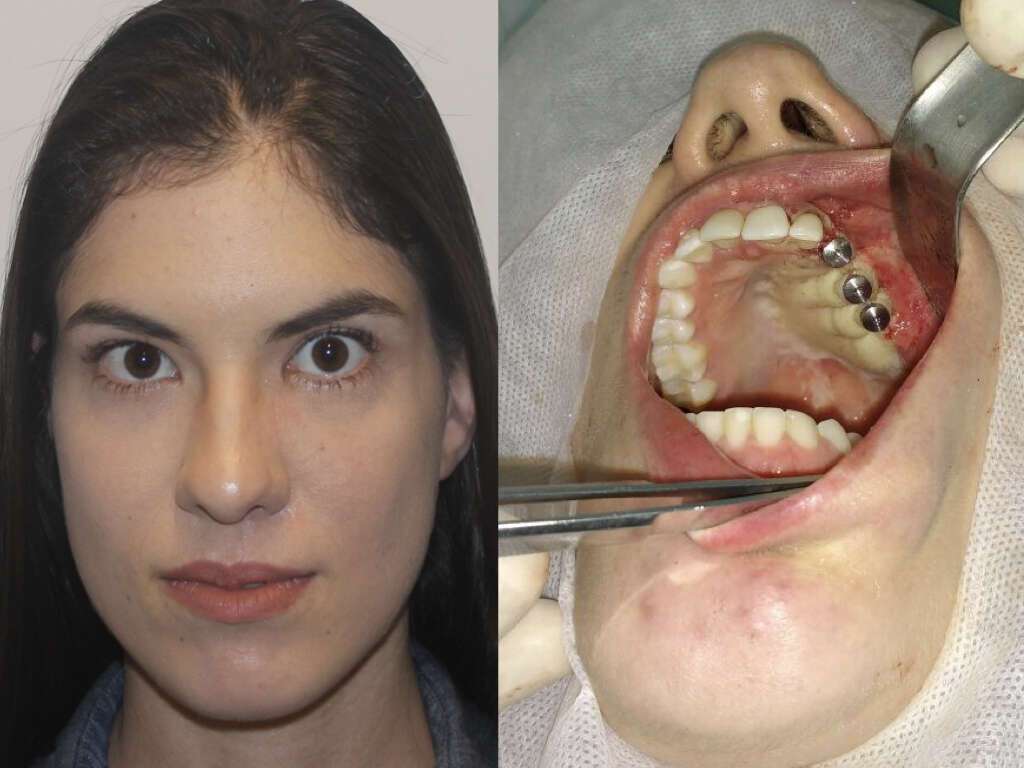
Immediate reconstruction was performed with a fibular osteomyocutaneous flap, anastomosed to the facial vessels. The bone element rebuilt the maxilla and alveolar ridge. Soft tissue portions of the flap replaced oral mucosa and nasal lining. Osteointegrated dental implants were inserted on the reconstructed fibula in a second procedure, improving functional outcome.
Patients required only 1 unit of blood transfusion and 3 days in ICU.
Results: Facial healing ocurred uneventfully as well as bone consolidation. Speech was normal after the procedure with adequate palate movement. Dental rehabilitation included a temporary dental cast followed by osteointegrated dental implants. No regrowth was observed after 2 years.
Conclusion: Adequate planning for resection of craniofacial AVM requires an integrated approach to allow proper diagnosis, radical resection and reconstruction. Aesthetically and functional recovery could be obtained in a single surgical procedure.


Powered by Eventact EMS