
Extracranial Arteriovenous Malformations: Prognostic Factors and Outcomes of Surgical Treatment in A Series of 67 Patients.
Objetives: Definitive treatment of extracranial arteriovenous malformations (AVM) is generally achieved by superselective embolization followed by surgical resection. Based on previous report, it seems that definition of limits on physical exam and extension of surgical resection may influence outcomes and regrowth rates. The objective of this study is to analyse a large series of patients to confirm this hypothesis.
Methods: Sixty-seven patients were surgically treated for head and neck AVMs between 2000 and 2018. Demographic data, perioperative information and characteristics of embolization procedures were collected. Craniofacial involvement was defined according to anatomic compromise (grades I-IV) and AVM limits were defined by clinical evaluation (definition of margins, well defined nidus and extension) as “precise” or “imprecise”. The type of resection was defined as complete or partial. Limits and type of resection were statistically analyzed looking for specific correlations. Fisher’s exact test and likelihood ratio test were used and a value of p ≤ 0.05 was considered significant.
Results: From the 67 cases, 38 were female. Regarding clinical evaluation, 39 patients had AVM with precise limits and 28 had imprecise limits. From the 67 cases, total resection was possible in 54 patients (37 with precise limits and 17 with imprecise limits).
After a mean follow-up of 4.5 years, the regrowth rate for the entire series was 23.8 percent (16 of 67 cases). Lesions with precise limits (p=0.015) and total surgical resection (p=0.001) were statistically associated with lower regrowth rates (table 1). The combination of incomplete resection and imprecise limits is the best explanation for rates of regrowth (p=0.010). Complete resection was the single most relevant parameter for favorable outcome.
Conclusion: Complete resection of extracranial AVM is the goal of every surgical procedure. When the nidus is well defined, a better prognosis is expected in the treatment of this group of patients.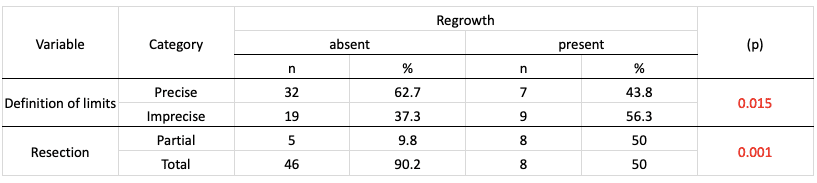
Powered by Eventact EMS