
Contrast Echocardiography to Exclude Active Intrapericardial Bleeding in Coronary Artery Perforation
A 66-year-old man underwent coronary angiography after detection of myocardial ischemia at stress test. Critical stenosis of the proximal segment of the ramus intermedius (RI) was detected. Wiring of the lesion was attempted using a Balance Middleweight Guidewire (Abbott Vascular, Santa Clara, CA), and subsequently using a Fielder XT-R and Sion Black (Asahi Intecc, Nagoya, Japan). Two Resolute Onyx stents (2.25x12 and 2.0x18 mm; Medtronic, Dublin, Ireland) were implanted at the proximal segment of the vessel. A 2.0x18 mm Resolute Onyx was then implanted because of a flow limiting dissection at the at the distal edge of the stent. Upon contrast injection, a distal type III CAP according to Ellis classification was evident. Prompt inflation of a semi-compliant balloon was performed. Hypotension and pulsus paradoxus arose. Transthoracic echocardiogram showed signs of cardiac tamponade. Emergent pericardial drainage was successfully performed. Embolization of the distal RI was performed through a right femoral approach (ping-pong technique) using three MicroNester 3 mm coils (Cook Medical, Bloomington, Indiana) delivered through a FineCross microcatheter (Terumo, Tokyo, Japan). The CAP was successfully sealed. After two hours, new signs of cardiac tamponade were evident requiring pericardial drainage. A second-look coronary angiography did not identify any active bleeding from the CAP. Therefore, contrast echocardiography was performed after the intravenous injection of 10 ml sodium hexafluoride-based ultrasound contrast (SonoVue, Bracco Imaging, San Donato Milanese, Italy), diluted at 50% and administered 2-3 ml at a time. No evidence of contrast in the pericardial space could be detected, ruling out active bleeding.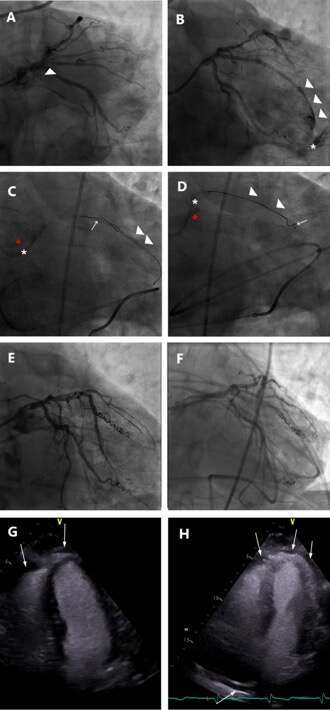
Powered by Eventact EMS