
Transseptal Removal of Fractured Guide Extension Catheter Using Deflectable Sheath
A 70-year-old female patient with severe mitral regurgitation after recent non-ST segment elevation myocardial infarction treated with single drug-eluting stent (DES) implantation to left main and circumflex was referred for percutaneous treatment of the remaining lesions in the heavily calcified LAD.
Successful percutaneous coronary intervention (PCI) with implantation of four DES to LM/LAD artery required the use of guide extension catheter (GEC) due to the calcified and tortuous LAD. GEC (Guidon, IMDS, Netherlands) was delivered with difficulties using protruding 3.0 mm balloon. An unexpected detachment of soft distal tip of the GEC (at the connection of the rapid exchange section and pushing rod) and its dislocation from guiding catheter to the left ventricle was observed during final angiography (a). The fracture occurred most likely due to considerable insertion forces and friction applied to GEC tip. Echocardiography imaging confirmed localization of the GEC in the left ventricle (LV) and left atrium (LA) (b). Angiographic imaging visualized presence of the radiopaque GEC tip in the left atrium (c).
The attempt to retrieve the GEC via trans-aortic approach using 7-Fr MPA catheter and gooseneck snare loop was unsuccessful. Therefore, we decided to use a trans-septal approach to recapture the dislocated GEC under fluoroscopic and transesophageal echocardiography guidance. An 8.5 deflectable Agilis sheath was introduced into the LA after a trans-septal puncture and the retrieval of the dislodged GEC was performed using a gooseneck snare loop (d). The GEC was successfully removed from the LA (e), which was confirmed in the final echocardiography (f).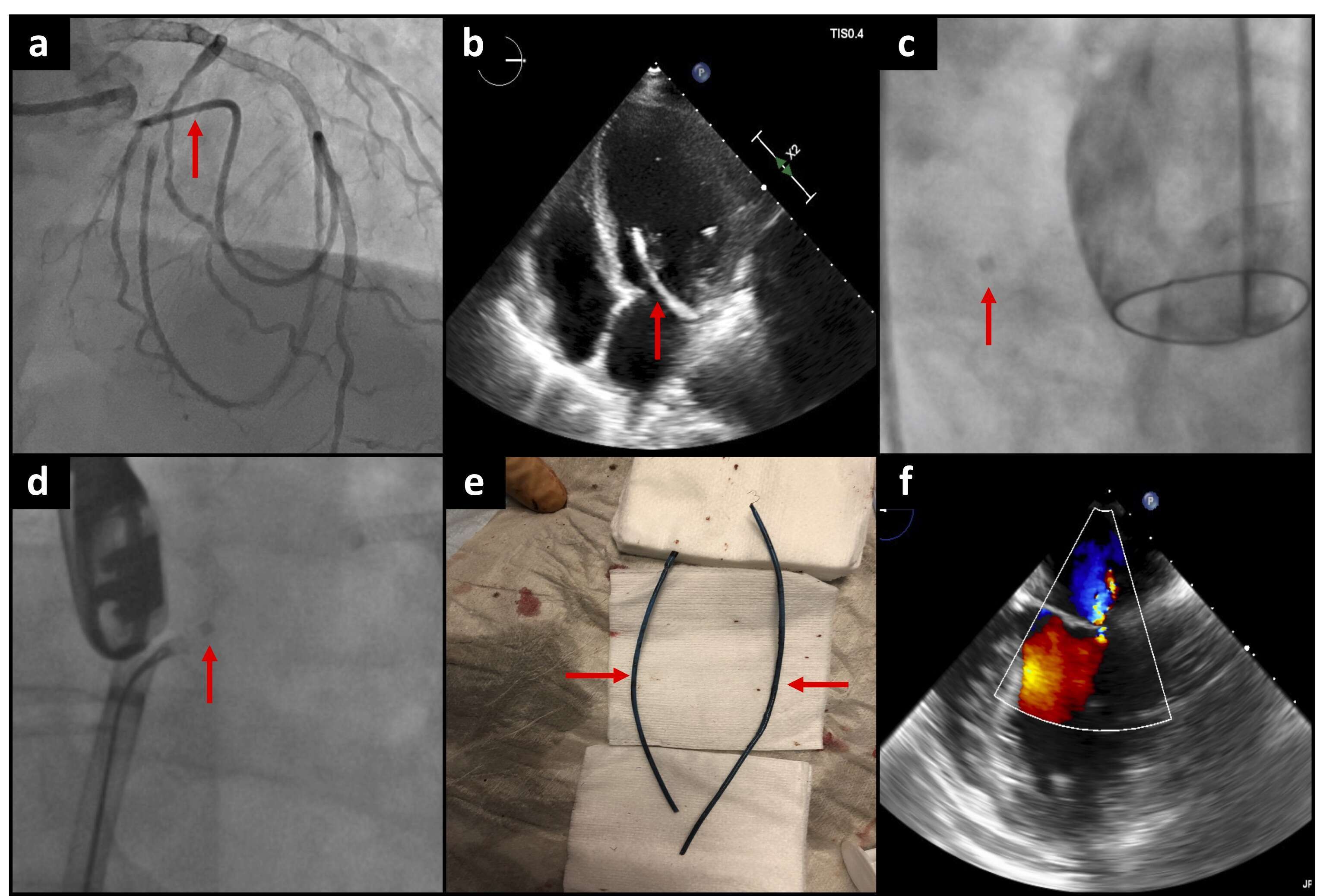
Powered by Eventact EMS